Monteggia Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes the condition of Monteggia fracture - ulna and radius.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Monteggia Fracture
Monteggia fracture is not a simple fracture. It is a fracture of the proximal ulna with dislocation of the radial head. Monteggia fracture can happen in children and in adults. It is one of the most common injuries that is missed in the emergency room in children. The radial head may be dislocated or subluxed, and this problem may not be clear on x-rays. If this injury is missed, then the child will probably need a big surgery to deal with this big problem. Treatment of this fracture depends on the age of the patient. In general, in pediatric patients, you will do closed reduction of the ulna and closed reduction of the radial head. In adult patients, you will do open reduction with internal fixation of the ulna with dorsal plate and closed reduction of the radial head. A line drawn from the proximal radius should bisect the capitellum in all x-ray views. If you are in doubt and not sure, get x-rays of the other side and compare. Always examine the patient for posterior interosseous nerve injury. The most common type is anterior Monteggia. That means that the apex of the fracture is anteriorly and the radial head goes anteriorly. Just make it a practice, when you have a fracture of the proximal ulna, look at the radius and the radial head, and see the position of the radial head in relationship to the capitellum. Anterior Monteggia is more common in children. Posterior Monteggia constitutes 70-80% of Monteggia fractures in adults. There are four types of Monteggia: Type I, Type II, Type III, and Type IV. Monteggia fracture is classified according to the direction of displacement of the radial head. The radial head has two relations: relation with the capitellum and relation with the proximal radioulnar joint. When the radial head subluxes or dislocates, it subluxes or dislocates from these two joints. The radial head becomes free. This means that the radius is not connected to the capitellum or to the superior radioulnar joint. A Type I fracture is of the middle or the proximal third of the ulna with anterior dislocation of the radial head, and it has the characteristic that the apex of the ulnar fracture is anteriorly. Type I fracture is the most common of all types (especially in children). Type I occurs in about 60% of fractures. In children, reduce the fractured ulna and reduce the dislocation of the radial head and immobilize the elbow in flexion and supination. When you flex the elbow, especially more than 90 degrees, you will relax the biceps (watch the circulation). A Type II fracture is a posterior type fracture. Posterior Monteggia is the most common type in adults. It is associated with a higher complication rate and carries the worst prognosis. 15% of Monteggia fractures are Type II. It is a fracture of the middle or proximal third of the ulna with posterior dislocation of the radial head. You should immobilize the elbow in extension. Type III is a lateral Monteggia. About 20% of Monteggia fractures are Type III. It is a fracture of the proximal ulna with lateral dislocation of the radial head. 5% of Monteggia fractures are Type IV; it is very rare. It is a fracture of the proximal ulna with anterior dislocation of the radial head and fracture of the proximal third of the radius below the bicipital tuberosity. The patient will need surgery, even in children. In this case, the radial head is dislocated, and you also have fractures of the radius and the ulna. The posterior interosseous nerve is adjacent to the radial neck, placing it at risk for a traction injury with dislocation of the proximal radius. You should do a neurovascular examination. A nerve injury which involves the posterior interosseous nerve is not uncommon. Ask the patient to “hitchhike” and extend their fingers. Make sure the wrist is in dorsiflexion when you ask the patient to extend the fingers. In posterior interosseous nerve injury, the finger extensors will not be working. If the posterior interosseous nerve is injured, observe the patient. In case of posterior interosseous nerve injury in Monteggia fracture, you will reduce and stabilize the fracture and reduce the radial head dislocation. Observe the nerve; do not explore the nerve. Typically the nerve injury is a neuropraxia. It can be expected to resolve itself with observation in 6-12 weeks. If it does not resolve, you will do EMG and nerve studies after that period of observation. Any time that you have an ulnar shaft fracture or any fracture of the proximal ulna, check the radial head position.
Видео Monteggia Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Monteggia Fracture
Monteggia fracture is not a simple fracture. It is a fracture of the proximal ulna with dislocation of the radial head. Monteggia fracture can happen in children and in adults. It is one of the most common injuries that is missed in the emergency room in children. The radial head may be dislocated or subluxed, and this problem may not be clear on x-rays. If this injury is missed, then the child will probably need a big surgery to deal with this big problem. Treatment of this fracture depends on the age of the patient. In general, in pediatric patients, you will do closed reduction of the ulna and closed reduction of the radial head. In adult patients, you will do open reduction with internal fixation of the ulna with dorsal plate and closed reduction of the radial head. A line drawn from the proximal radius should bisect the capitellum in all x-ray views. If you are in doubt and not sure, get x-rays of the other side and compare. Always examine the patient for posterior interosseous nerve injury. The most common type is anterior Monteggia. That means that the apex of the fracture is anteriorly and the radial head goes anteriorly. Just make it a practice, when you have a fracture of the proximal ulna, look at the radius and the radial head, and see the position of the radial head in relationship to the capitellum. Anterior Monteggia is more common in children. Posterior Monteggia constitutes 70-80% of Monteggia fractures in adults. There are four types of Monteggia: Type I, Type II, Type III, and Type IV. Monteggia fracture is classified according to the direction of displacement of the radial head. The radial head has two relations: relation with the capitellum and relation with the proximal radioulnar joint. When the radial head subluxes or dislocates, it subluxes or dislocates from these two joints. The radial head becomes free. This means that the radius is not connected to the capitellum or to the superior radioulnar joint. A Type I fracture is of the middle or the proximal third of the ulna with anterior dislocation of the radial head, and it has the characteristic that the apex of the ulnar fracture is anteriorly. Type I fracture is the most common of all types (especially in children). Type I occurs in about 60% of fractures. In children, reduce the fractured ulna and reduce the dislocation of the radial head and immobilize the elbow in flexion and supination. When you flex the elbow, especially more than 90 degrees, you will relax the biceps (watch the circulation). A Type II fracture is a posterior type fracture. Posterior Monteggia is the most common type in adults. It is associated with a higher complication rate and carries the worst prognosis. 15% of Monteggia fractures are Type II. It is a fracture of the middle or proximal third of the ulna with posterior dislocation of the radial head. You should immobilize the elbow in extension. Type III is a lateral Monteggia. About 20% of Monteggia fractures are Type III. It is a fracture of the proximal ulna with lateral dislocation of the radial head. 5% of Monteggia fractures are Type IV; it is very rare. It is a fracture of the proximal ulna with anterior dislocation of the radial head and fracture of the proximal third of the radius below the bicipital tuberosity. The patient will need surgery, even in children. In this case, the radial head is dislocated, and you also have fractures of the radius and the ulna. The posterior interosseous nerve is adjacent to the radial neck, placing it at risk for a traction injury with dislocation of the proximal radius. You should do a neurovascular examination. A nerve injury which involves the posterior interosseous nerve is not uncommon. Ask the patient to “hitchhike” and extend their fingers. Make sure the wrist is in dorsiflexion when you ask the patient to extend the fingers. In posterior interosseous nerve injury, the finger extensors will not be working. If the posterior interosseous nerve is injured, observe the patient. In case of posterior interosseous nerve injury in Monteggia fracture, you will reduce and stabilize the fracture and reduce the radial head dislocation. Observe the nerve; do not explore the nerve. Typically the nerve injury is a neuropraxia. It can be expected to resolve itself with observation in 6-12 weeks. If it does not resolve, you will do EMG and nerve studies after that period of observation. Any time that you have an ulnar shaft fracture or any fracture of the proximal ulna, check the radial head position.
Видео Monteggia Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Galeazzi Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Galeazzi Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Monteggia Vs. Galeazzi fracture
Monteggia Vs. Galeazzi fracture Supracondylar Fractures Of The Humerus In Children
Supracondylar Fractures Of The Humerus In Children Ligaments of the Elbow Stability Of The Elbow - Everything You Need To Know - Dr. Nabil Ebraheim
Ligaments of the Elbow Stability Of The Elbow - Everything You Need To Know - Dr. Nabil Ebraheim Osteomyelitis Bone Infection - Everything You Need To Know - Dr. Nabil Ebraheim
Osteomyelitis Bone Infection - Everything You Need To Know - Dr. Nabil Ebraheim Named Fractures: UPPER LIMB, Fractures with EPONYMS, NEET PG, The Young Orthopod
Named Fractures: UPPER LIMB, Fractures with EPONYMS, NEET PG, The Young Orthopod Monteggia Fractures In Children
Monteggia Fractures In Children Interosseous Muscles Of The Hand Anatomy - Everything You Need To Know - Dr. Nabil Ebraheim
Interosseous Muscles Of The Hand Anatomy - Everything You Need To Know - Dr. Nabil Ebraheim Perilunate Instability & Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim
Perilunate Instability & Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim Acetabular Fracture Radiographic Evaluation - Everything You Need To Know - Dr. Nabil Ebraheim
Acetabular Fracture Radiographic Evaluation - Everything You Need To Know - Dr. Nabil Ebraheim Dislocation of the hip - Everything You Need To Know - Dr. Nabil Ebraheim
Dislocation of the hip - Everything You Need To Know - Dr. Nabil Ebraheim Radius & Ulnar Shaft Fracture Approaches - Everything You Need To Know - Dr. Nabil Ebraheim
Radius & Ulnar Shaft Fracture Approaches - Everything You Need To Know - Dr. Nabil Ebraheim Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim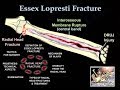 Fracture Of The Radial Head Essex Lopresti - Everything You Need To Know - Dr. Nabil Ebraheim
Fracture Of The Radial Head Essex Lopresti - Everything You Need To Know - Dr. Nabil Ebraheim Biceps Tendonitis - Everything You Need To Know - Dr. Nabil Ebraheim
Biceps Tendonitis - Everything You Need To Know - Dr. Nabil Ebraheim Fracture Healing - Everything You Need To Know - Dr. Nabil Ebraheim
Fracture Healing - Everything You Need To Know - Dr. Nabil Ebraheim Sternoclavicular Joint Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
Sternoclavicular Joint Injuries - Everything You Need To Know - Dr. Nabil Ebraheim Pediatric fractures ,Upper Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim
Pediatric fractures ,Upper Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim Monteggia Fracture Dislocation
Monteggia Fracture Dislocation Elbow Dislocation In Adults - Everything You Need To Know - Dr. Nabil Ebraheim
Elbow Dislocation In Adults - Everything You Need To Know - Dr. Nabil Ebraheim