Pediatric fractures ,Upper Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video about Pediatric Upper Extremity.
Fracture of the proximal end of the clavicle is considered to be a physeal growth plate injury and not a sternoclavicular joint injury, especially if it occurs in patients younger than 25 years of age. The proximal (medial) clavicle epiphysis is the last to fuse.
The distal clavicle fracture is usually a sleeve fracture that resembles an AC joint separation. Diaphyseal fractures in children are common in the middle third of the clavicle. Diaphyseal fractures usually heal with an excellent remodeling ability within one year.
Clavicle birth fractures usually occur when the baby is large. The baby may have pseudoparalysis and is treated with a sling or simple immobilization. You will need to do differential diagnosis between brachial plexus injury and a clavicle fracture.
Watch out for fractures of the clavicle in the mid-shaft area that could be congenital pseudoarthrosis. The condition is treated conservatively. Congenital pseudoarthrosis is usually on the right side and asymptomatic. If the child is symptomatic and older, treat it with a fixation and bone graft.
Next is the proximal humerus. 80% of the longitudinal growth of the humerus occurs in the proximal physis. In young children, fractures are treated conservatively with a sling and the patient may get a hanging arm cast. Try to get upright x-rays. Remember! In a young child, proximal humerus fractures allow for significant remodeling following injury of the proximal physis, even if the fracture is badly displaced. Treat is conservatively. In older children, closed reduction and percutaneous pinning may be needed, especially if there is a major displacement.
The “little leaguer’s shoulder” is a widened growth plate of the proximal humerus and it is considered to be a stress fracture due to overuse. Treatment of little leaguer’s shoulder consists of cessation of throwing and a period of rest.
Next we will discuss elbow fractures. The first one is transepiphyseal separation of the distal humerus. Consider child abuse in these injuries! It is usually confused with elbow dislocations, however the radiocapitellar line remains the same. The olecranon moves posteriorly and medially. Physeal separation of the distal humerus usually occurs in younger ages. The diagnosis is usually difficult and may be missed. There separations should be highly suspected with elbow injuries before the age of 1 year.
What are other findings that may be a sign of child abuse?
Child abuse should be considered if the patient has multiple fractures at different stages of healing, corner fractures, posterior rib fractures or fracture of the femur before they are of walking age.
There is a mnemonic statement that can be used to remember the names and order of the elbow ossification centers: CRITOE. This is the ages when the ossification centers appear around the elbow.
The ossification center appears around the capitellum at 1 year. The ossification center appears around the radial head at 3 years. The ossification center around the internal epicondyle (medial) appears at 5 years. The ossification center appears around the trochlea at 7 years. The ossification center around the olecranon appears at 9 years. Lastly, the ossification center around the external epicondyle (lateral) appears at 11 years.
Lateral condylar fractures are most commonly Salter-Harris Type IV fractures. If the fracture appears to be nondisplaced, you need to get an internal rotation oblique view x-ray that will show the fracture displacement better. Watch the fracture to make sure that it does not displace. Surgery should be done if the fracture is displaced. When surgery is done, it needs to be done with a lateral approach and not a posterior approach due to the risk of injury to the blood supply of the capitellum, which could cause avascular necrosis. Some may use arthrogram or a percutaneous technique. It is better to open through a lateral approach, especially if the fracture is badly displaced.
The complications associated with lateral condylar fractures and nonunion and you can have cubitus valgus and ulnar nerve symptoms. It takes years to develop ulnar nerve symptoms. If there is good motion of the elbow but there is pain, then we need to do bone graft and fixation. If there are ulnar symptoms, then you need to release or transpose the ulnar nerve. There is no question that lateral condylar fractures are a surgical case!
The medial epicondyle growth plate is the last one to fuse. The “little leaguer’s elbow” is caused by a pitching motion which places stress on the elbow joint, resulting in avulsion and inflammation of the medial epicondylar apophysis. Fracture of the medial epicondyle is usually treated conservatively.
Видео Pediatric fractures ,Upper Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Fracture of the proximal end of the clavicle is considered to be a physeal growth plate injury and not a sternoclavicular joint injury, especially if it occurs in patients younger than 25 years of age. The proximal (medial) clavicle epiphysis is the last to fuse.
The distal clavicle fracture is usually a sleeve fracture that resembles an AC joint separation. Diaphyseal fractures in children are common in the middle third of the clavicle. Diaphyseal fractures usually heal with an excellent remodeling ability within one year.
Clavicle birth fractures usually occur when the baby is large. The baby may have pseudoparalysis and is treated with a sling or simple immobilization. You will need to do differential diagnosis between brachial plexus injury and a clavicle fracture.
Watch out for fractures of the clavicle in the mid-shaft area that could be congenital pseudoarthrosis. The condition is treated conservatively. Congenital pseudoarthrosis is usually on the right side and asymptomatic. If the child is symptomatic and older, treat it with a fixation and bone graft.
Next is the proximal humerus. 80% of the longitudinal growth of the humerus occurs in the proximal physis. In young children, fractures are treated conservatively with a sling and the patient may get a hanging arm cast. Try to get upright x-rays. Remember! In a young child, proximal humerus fractures allow for significant remodeling following injury of the proximal physis, even if the fracture is badly displaced. Treat is conservatively. In older children, closed reduction and percutaneous pinning may be needed, especially if there is a major displacement.
The “little leaguer’s shoulder” is a widened growth plate of the proximal humerus and it is considered to be a stress fracture due to overuse. Treatment of little leaguer’s shoulder consists of cessation of throwing and a period of rest.
Next we will discuss elbow fractures. The first one is transepiphyseal separation of the distal humerus. Consider child abuse in these injuries! It is usually confused with elbow dislocations, however the radiocapitellar line remains the same. The olecranon moves posteriorly and medially. Physeal separation of the distal humerus usually occurs in younger ages. The diagnosis is usually difficult and may be missed. There separations should be highly suspected with elbow injuries before the age of 1 year.
What are other findings that may be a sign of child abuse?
Child abuse should be considered if the patient has multiple fractures at different stages of healing, corner fractures, posterior rib fractures or fracture of the femur before they are of walking age.
There is a mnemonic statement that can be used to remember the names and order of the elbow ossification centers: CRITOE. This is the ages when the ossification centers appear around the elbow.
The ossification center appears around the capitellum at 1 year. The ossification center appears around the radial head at 3 years. The ossification center around the internal epicondyle (medial) appears at 5 years. The ossification center appears around the trochlea at 7 years. The ossification center around the olecranon appears at 9 years. Lastly, the ossification center around the external epicondyle (lateral) appears at 11 years.
Lateral condylar fractures are most commonly Salter-Harris Type IV fractures. If the fracture appears to be nondisplaced, you need to get an internal rotation oblique view x-ray that will show the fracture displacement better. Watch the fracture to make sure that it does not displace. Surgery should be done if the fracture is displaced. When surgery is done, it needs to be done with a lateral approach and not a posterior approach due to the risk of injury to the blood supply of the capitellum, which could cause avascular necrosis. Some may use arthrogram or a percutaneous technique. It is better to open through a lateral approach, especially if the fracture is badly displaced.
The complications associated with lateral condylar fractures and nonunion and you can have cubitus valgus and ulnar nerve symptoms. It takes years to develop ulnar nerve symptoms. If there is good motion of the elbow but there is pain, then we need to do bone graft and fixation. If there are ulnar symptoms, then you need to release or transpose the ulnar nerve. There is no question that lateral condylar fractures are a surgical case!
The medial epicondyle growth plate is the last one to fuse. The “little leaguer’s elbow” is caused by a pitching motion which places stress on the elbow joint, resulting in avulsion and inflammation of the medial epicondylar apophysis. Fracture of the medial epicondyle is usually treated conservatively.
Видео Pediatric fractures ,Upper Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Supracondylar Fractures Of The Humerus In Children
Supracondylar Fractures Of The Humerus In Children NERVE INJURY IN THE UPPER EXTREMITY- Everything You Need To Know - Dr. Nabil Ebraheim
NERVE INJURY IN THE UPPER EXTREMITY- Everything You Need To Know - Dr. Nabil Ebraheim Named Fractures: UPPER LIMB, Fractures with EPONYMS, NEET PG, The Young Orthopod
Named Fractures: UPPER LIMB, Fractures with EPONYMS, NEET PG, The Young Orthopod Arteries of the upper limb
Arteries of the upper limb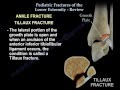 Pediatric Fractures Of The Lower Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim
Pediatric Fractures Of The Lower Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim Overview Of Fractures In The Pediatric Age Group
Overview Of Fractures In The Pediatric Age Group Supracondylar humerus fracture , pulseless hand - Everything You Need To Know - Dr. Nabil Ebraheim
Supracondylar humerus fracture , pulseless hand - Everything You Need To Know - Dr. Nabil Ebraheim ORTHO at a GLANCE - Upper Limb
ORTHO at a GLANCE - Upper Limb Humerus, Distal—Lateral Condyle and Medial Epicondyle Fractures
Humerus, Distal—Lateral Condyle and Medial Epicondyle Fractures Imaging & Low Back Pain - Everything You Need To Know - Dr. Nabil Ebraheim
Imaging & Low Back Pain - Everything You Need To Know - Dr. Nabil Ebraheim Principles of Fracture Fixation | Orthopedic Basics
Principles of Fracture Fixation | Orthopedic Basics FRACTURES OF UPPER LIMB |CLAVICLE | SHOULDER JOINT DISLOCATION|
FRACTURES OF UPPER LIMB |CLAVICLE | SHOULDER JOINT DISLOCATION| Hip Fractures Surgical Fixation - Everything You Need To Know - Dr. Nabil Ebraheim
Hip Fractures Surgical Fixation - Everything You Need To Know - Dr. Nabil Ebraheim Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Rotator Cuff tear Imaging - Everything You Need To Know - Dr. Nabil Ebraheim
Rotator Cuff tear Imaging - Everything You Need To Know - Dr. Nabil Ebraheim Symptoms Of Spine Problems - Everything You Need To Know - Dr. Nabil Ebraheim
Symptoms Of Spine Problems - Everything You Need To Know - Dr. Nabil Ebraheim Elbow muscles (anatomy)
Elbow muscles (anatomy) Achilles Tendon Rupture - Everything You Need To Know - Dr. Nabil Ebraheim
Achilles Tendon Rupture - Everything You Need To Know - Dr. Nabil Ebraheim Fractures & Dislocations of Upper Limb | Orthopaedic
Fractures & Dislocations of Upper Limb | Orthopaedic Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim
Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim