Supracondylar humerus fracture , pulseless hand - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video supracondylar fracture of the humerus in children.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
View my profile on Linkedin:
https://www.linkedin.com/in/nabilebraheim/
Vascular compromise in displaced supracondylar humerus fractures can be present in up to 20% of patients usually due to brachial artery injury. Fracture displacement may cause injury to the surrounding soft tissue, including the brachial artery and the radial or median nerve, with reported incidence as high as 50%. Complete median nerve injury deficit is a predictive of brachial artery injury. In extension injury, the anterior interosseous nerve can be injured and the child will not be able to do the O.K. sign. In flexion type injury, and ulnar nerve injury may occur (the patient may get ulnar nerve palsy). The brachial artery can be stretched or kinked over the displaced fracture fragments. It can be tethered by the ulnar sided supratrochlear branch of the brachial artery. Nerve injuries in general can occur in about 10-20% of supracondylar humeral fractures. It is usually a traction nueropraxia that will improve with time. Do observation for the patient. Due to the anatomic proximity of the median nerve to the brachial artery, injury to one structure may predict injury to the other. Median nerve injury in displaced supracondylar humeral fracture may suggest vascular injury as well as a pulseless limb. The physician should perform a careful neurovascular exam in patients with supracondylar humeral fractures. In the initial exam, the physician should establish if it is a nerve injury, if there is a distal pulse (usually the radial pulse is palpated) and if the hand is pink. Check for nerve injury, a distal pulse, and a pink hand. Examination findings of the injured extremity should be compared with the other side (noninjured side). Supracondylar humeral fractures with an absent radial pulse and a median nerve injury should raise suspicion for an associated vascular injury. To assess the vascular status, assess the radial artery, hand color, temperature and edema, capillary refill compared to the other side, and pain level. If there is an increase in analgesic requirement, this may indicate the development of a compartment syndrome. It is generally accepted that arterial capillary refill should be less than 2 seconds, and this should be compared with the other side. Prolonged arterial capillary refill, pulselessness, diminished digital pulp turgor, cooler hand temperature, palor and severe edema may be signs of a poorly perfused limb. Clinical findings of vascular injury include high energy injury, antecubital ecchymosis, and puckering of the anterior skin. When there is a displaced fracture, we have to be suspicious of the development of compartment syndrome. There is a high incidence of compartment syndrome with Type III fractures. In Type III fractures, the volar forearm compartment pressures are on an average 5-19 mmHg higher than those of Type II fractures. If the limb is dysvascular for greater than 6 hours, prophylactic volar compartment release should be done. Some believe that prophylactic fasciotomy should be done if there is a vascular injury that required repair. The clinician should attempt to improve the position of al ldisplaced supracondylar fractures of the humerus. You will need to do gentle traction and flex the elbow from 30-45 degrees and immobilize the elbow in a posterior splint. This maneuver may improve the position of the fracture and may restore the pulse, improve the circulation and the perfusion with very little risk of causing harm to the patient. Do not flex the elbow excessively because it can impair the circulation even more. Signs of distal ischemia are usually a cool, pale hand. If you have a pulseless, poorly perfused limb after gentle traction in a splint, then you will need to do emergency surgery. You will do operative reduction of the fracture (closed or open) and pinning. The pulses and the perfusion is usually restored in about 53-70 percent of patients, and if the pulses and perfusion were not restored, then you will do immediate open vascular exploration. The chance of brachial artery injury is as high as 80%. If you do an open exploration and reduction, you will do a 4-5cm transverse anterior incision in the antecubital flexion crease. Then you will do decompression of the artery and repair of the artery with reverse vein graft. If the hand is pink and pulseless, this is usually due to transient brachial arterial spasm or it may be due to brachial artery injury with the distal perfusion maintained by rich collateral circulation at the elbow. You may increase the ambient temperature in the operating room and apply a topical agent such as lidocaine or papverine which allows resolution of the vasospasm and restoration of the distal arterial flow.
Видео Supracondylar humerus fracture , pulseless hand - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
View my profile on Linkedin:
https://www.linkedin.com/in/nabilebraheim/
Vascular compromise in displaced supracondylar humerus fractures can be present in up to 20% of patients usually due to brachial artery injury. Fracture displacement may cause injury to the surrounding soft tissue, including the brachial artery and the radial or median nerve, with reported incidence as high as 50%. Complete median nerve injury deficit is a predictive of brachial artery injury. In extension injury, the anterior interosseous nerve can be injured and the child will not be able to do the O.K. sign. In flexion type injury, and ulnar nerve injury may occur (the patient may get ulnar nerve palsy). The brachial artery can be stretched or kinked over the displaced fracture fragments. It can be tethered by the ulnar sided supratrochlear branch of the brachial artery. Nerve injuries in general can occur in about 10-20% of supracondylar humeral fractures. It is usually a traction nueropraxia that will improve with time. Do observation for the patient. Due to the anatomic proximity of the median nerve to the brachial artery, injury to one structure may predict injury to the other. Median nerve injury in displaced supracondylar humeral fracture may suggest vascular injury as well as a pulseless limb. The physician should perform a careful neurovascular exam in patients with supracondylar humeral fractures. In the initial exam, the physician should establish if it is a nerve injury, if there is a distal pulse (usually the radial pulse is palpated) and if the hand is pink. Check for nerve injury, a distal pulse, and a pink hand. Examination findings of the injured extremity should be compared with the other side (noninjured side). Supracondylar humeral fractures with an absent radial pulse and a median nerve injury should raise suspicion for an associated vascular injury. To assess the vascular status, assess the radial artery, hand color, temperature and edema, capillary refill compared to the other side, and pain level. If there is an increase in analgesic requirement, this may indicate the development of a compartment syndrome. It is generally accepted that arterial capillary refill should be less than 2 seconds, and this should be compared with the other side. Prolonged arterial capillary refill, pulselessness, diminished digital pulp turgor, cooler hand temperature, palor and severe edema may be signs of a poorly perfused limb. Clinical findings of vascular injury include high energy injury, antecubital ecchymosis, and puckering of the anterior skin. When there is a displaced fracture, we have to be suspicious of the development of compartment syndrome. There is a high incidence of compartment syndrome with Type III fractures. In Type III fractures, the volar forearm compartment pressures are on an average 5-19 mmHg higher than those of Type II fractures. If the limb is dysvascular for greater than 6 hours, prophylactic volar compartment release should be done. Some believe that prophylactic fasciotomy should be done if there is a vascular injury that required repair. The clinician should attempt to improve the position of al ldisplaced supracondylar fractures of the humerus. You will need to do gentle traction and flex the elbow from 30-45 degrees and immobilize the elbow in a posterior splint. This maneuver may improve the position of the fracture and may restore the pulse, improve the circulation and the perfusion with very little risk of causing harm to the patient. Do not flex the elbow excessively because it can impair the circulation even more. Signs of distal ischemia are usually a cool, pale hand. If you have a pulseless, poorly perfused limb after gentle traction in a splint, then you will need to do emergency surgery. You will do operative reduction of the fracture (closed or open) and pinning. The pulses and the perfusion is usually restored in about 53-70 percent of patients, and if the pulses and perfusion were not restored, then you will do immediate open vascular exploration. The chance of brachial artery injury is as high as 80%. If you do an open exploration and reduction, you will do a 4-5cm transverse anterior incision in the antecubital flexion crease. Then you will do decompression of the artery and repair of the artery with reverse vein graft. If the hand is pink and pulseless, this is usually due to transient brachial arterial spasm or it may be due to brachial artery injury with the distal perfusion maintained by rich collateral circulation at the elbow. You may increase the ambient temperature in the operating room and apply a topical agent such as lidocaine or papverine which allows resolution of the vasospasm and restoration of the distal arterial flow.
Видео Supracondylar humerus fracture , pulseless hand - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Supracondylar Fractures Of The Humerus In Children
Supracondylar Fractures Of The Humerus In Children Pediatric fractures ,Upper Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim
Pediatric fractures ,Upper Extremity Review - Everything You Need To Know - Dr. Nabil Ebraheim Supracondylar fracture - radiology video tutorial (x-ray)
Supracondylar fracture - radiology video tutorial (x-ray) Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Acute and chronic leg Compartment Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim
Acute and chronic leg Compartment Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim Radial Nerve Injury,Where Is The Injury - Everything You Need To Know - Dr. Nabil Ebraheim
Radial Nerve Injury,Where Is The Injury - Everything You Need To Know - Dr. Nabil Ebraheim Genu Valgus - Dr Ravi Chauhan
Genu Valgus - Dr Ravi Chauhan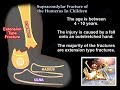 Supracondylar Fracture Of The Humerus In Children - Everything You Need To Know - Dr. Nabil Ebraheim
Supracondylar Fracture Of The Humerus In Children - Everything You Need To Know - Dr. Nabil Ebraheim Sternoclavicular Joint Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
Sternoclavicular Joint Injuries - Everything You Need To Know - Dr. Nabil Ebraheim Lumbar Spinal Stenosis - Everything You Need To Know - Dr. Nabil Ebraheim
Lumbar Spinal Stenosis - Everything You Need To Know - Dr. Nabil Ebraheim Humerus
Humerus Osteomyelitis Bone Infection - Everything You Need To Know - Dr. Nabil Ebraheim
Osteomyelitis Bone Infection - Everything You Need To Know - Dr. Nabil Ebraheim Spinal Cord Injury, Detailed - Everything You Need To Know - Dr. Nabil Ebraheim
Spinal Cord Injury, Detailed - Everything You Need To Know - Dr. Nabil Ebraheim Monteggia Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Monteggia Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Scaphoid Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Scaphoid Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Supracondylar Fracture Humerus & Circulation - Everything You Need To Know - Dr. Nabil Ebraheim
Supracondylar Fracture Humerus & Circulation - Everything You Need To Know - Dr. Nabil Ebraheim The Baxter's Nerve - Everything You Need To Know - Dr. Nabil Ebraheim
The Baxter's Nerve - Everything You Need To Know - Dr. Nabil Ebraheim Proximal Humerus Fractures classification - Everything You Need To Know - Dr. Nabil Ebraheim
Proximal Humerus Fractures classification - Everything You Need To Know - Dr. Nabil Ebraheim Gluteus Medius Tendon Tear - Everything You Need To Know - Dr. Nabil Ebraheim
Gluteus Medius Tendon Tear - Everything You Need To Know - Dr. Nabil Ebraheim Posterior Labral Tear Shoulder Instability - Everything You Need To Know - Dr. Nabil Ebraheim
Posterior Labral Tear Shoulder Instability - Everything You Need To Know - Dr. Nabil Ebraheim