Dislocation of the hip - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes types of hip dislocations.
Hip dislocation cab be either a simple dislocation or it can be a fracture dislocation which involves the posterior wall of the acetabulum or the femoral head.
Dislocation of the hip can be two types:
1.Posterior dislocation (most common type)
2.Anterior dislocation (rare)
Position of the hip during the impact decides the injury.
In posterior dislocation of the hip, which is the most common type, the lower limb will be flexed, adducted and internally rotated.
Hip fractures are different than hip dislocations. Notice that the affected extremity is shortened and externally rotated with a hip fracture.
Hip dislocation of any type is an emergency. It must be reduced in less than 6 hours of injury. After reduction of the hip, get a CT scan. A CT scan clearly outlines the bony injury. Check the CT scan for congruous reduction, for the absence of fracture and absence of marginal impaction in the acetabulum. Marginal impaction is more common in posterior acetabular wall fractures and could lead to instability.
Displaced or comminuted posterior wall fracture could lead to arthritis. Make sure that you have a congruous reduction with no loose bodies or important fractures present. Check for fractures of the acetabulum and the size of the fragment. The size of the posterior wall fracture has an effect on the stability of the hip joint. If congruous reduction of the hip is not obtained, perform open reduction urgently. Open reduction can be done through an anterior approach or a posterior approach.
Hip dislocation with or without associated fracture can cause complications.The risk of avascular necrosis depends on the interval between the injury and reduction of the dislocation. Urgent reduction of hip dislocation is mandatory to avoid AVN and interruption of the blood supply which leads to collapse of the femoral head. Closed reduction should be done in less than 6 hours.
When injury occurs to the sciatic nerve due to posterior hip dislocation, the common peroneal nerve is usually affected, causing weakness in dorsiflexion of the ankle and loss of toe extension.
Injury to the sciatic nerve usually occurs from the dislocation and not from the reduction of the hip. The longer the wait for the reduction of the dislocation, the more the patient is predisposed to sciatic nerve injury. The length of time a hip remains dislocated influences the incidence and the severity of a major sciatic nerve injury.
Neurological examination at the time of injury is usually difficult, however it is extremely necessary. Check for sensation on the top of the foot.
In posterior dislocation of the hip, always look for injuries in the knee such as dashboard injury. The force of the injury is usually transmitted from the knee to the hip.
In cases of high energy trauma, always look at the chest. There might be a tear of the aorta. Check for widening of the mediastinum on chest x-rays. There is concern of deceleration injury involving the aorta.
Hip joint dislocation may be associated with acetabular fracture or fracture of the femoral head (Pipkin fracture). With Pipkin fracture, as the femoral head dislocated, it hits the posterior wall of the acetabulum and the femoral head fractures. This may be different from an anterior hip dislocation. Anterior hip dislocation will cause impaction of the femoral head or indentation fractures. Classically, Pipkin fracture is a posterior fracture dislocation of the hip and fracture of the femoral head.
Treatment of hip dislocation
•Emergency closed reduction of the hip within 6 hours.
•Closed reduction is done to avoid AVN of the hip.
•Reduction of the hip joint and mobilization of the patient with protected weight-bearing crutches for 4-6 weeks.
•After closed reduction, when the patient has an associated fracture, assess the ip stability
•The hip is usually stable if the fragment size of the acetabulum is less than 20% •More than 40 %, the hip is unstable. •Between 20-40% fragment size, the hip stability is undetermined.
When there is an associated acetabular fracture, the best method to assess the stability of the hip is by examination of the patient under general anesthesia utilizing fluoroscopy.
Assess the posterior wall stability with the obturator oblique view. Hip will be in flexion, adduction and add axial load. Check the medial clear space for opening.
Irreducible isolated posterior dislocation
•Do emergency surgical treatment to reduce the hip.
Treatment of posterior hip dislocation with posterior acetabular wall fracture
•Must assess the stability of the hip joint by examination under anesthesia after closed reduction.
•After closed reduction, if the dislocation is not congruent, do open reduction and fixation urgently.
Treatment of Pipkin femoral head fractures
•Headless screw fixation.
Видео Dislocation of the hip - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Hip dislocation cab be either a simple dislocation or it can be a fracture dislocation which involves the posterior wall of the acetabulum or the femoral head.
Dislocation of the hip can be two types:
1.Posterior dislocation (most common type)
2.Anterior dislocation (rare)
Position of the hip during the impact decides the injury.
In posterior dislocation of the hip, which is the most common type, the lower limb will be flexed, adducted and internally rotated.
Hip fractures are different than hip dislocations. Notice that the affected extremity is shortened and externally rotated with a hip fracture.
Hip dislocation of any type is an emergency. It must be reduced in less than 6 hours of injury. After reduction of the hip, get a CT scan. A CT scan clearly outlines the bony injury. Check the CT scan for congruous reduction, for the absence of fracture and absence of marginal impaction in the acetabulum. Marginal impaction is more common in posterior acetabular wall fractures and could lead to instability.
Displaced or comminuted posterior wall fracture could lead to arthritis. Make sure that you have a congruous reduction with no loose bodies or important fractures present. Check for fractures of the acetabulum and the size of the fragment. The size of the posterior wall fracture has an effect on the stability of the hip joint. If congruous reduction of the hip is not obtained, perform open reduction urgently. Open reduction can be done through an anterior approach or a posterior approach.
Hip dislocation with or without associated fracture can cause complications.The risk of avascular necrosis depends on the interval between the injury and reduction of the dislocation. Urgent reduction of hip dislocation is mandatory to avoid AVN and interruption of the blood supply which leads to collapse of the femoral head. Closed reduction should be done in less than 6 hours.
When injury occurs to the sciatic nerve due to posterior hip dislocation, the common peroneal nerve is usually affected, causing weakness in dorsiflexion of the ankle and loss of toe extension.
Injury to the sciatic nerve usually occurs from the dislocation and not from the reduction of the hip. The longer the wait for the reduction of the dislocation, the more the patient is predisposed to sciatic nerve injury. The length of time a hip remains dislocated influences the incidence and the severity of a major sciatic nerve injury.
Neurological examination at the time of injury is usually difficult, however it is extremely necessary. Check for sensation on the top of the foot.
In posterior dislocation of the hip, always look for injuries in the knee such as dashboard injury. The force of the injury is usually transmitted from the knee to the hip.
In cases of high energy trauma, always look at the chest. There might be a tear of the aorta. Check for widening of the mediastinum on chest x-rays. There is concern of deceleration injury involving the aorta.
Hip joint dislocation may be associated with acetabular fracture or fracture of the femoral head (Pipkin fracture). With Pipkin fracture, as the femoral head dislocated, it hits the posterior wall of the acetabulum and the femoral head fractures. This may be different from an anterior hip dislocation. Anterior hip dislocation will cause impaction of the femoral head or indentation fractures. Classically, Pipkin fracture is a posterior fracture dislocation of the hip and fracture of the femoral head.
Treatment of hip dislocation
•Emergency closed reduction of the hip within 6 hours.
•Closed reduction is done to avoid AVN of the hip.
•Reduction of the hip joint and mobilization of the patient with protected weight-bearing crutches for 4-6 weeks.
•After closed reduction, when the patient has an associated fracture, assess the ip stability
•The hip is usually stable if the fragment size of the acetabulum is less than 20% •More than 40 %, the hip is unstable. •Between 20-40% fragment size, the hip stability is undetermined.
When there is an associated acetabular fracture, the best method to assess the stability of the hip is by examination of the patient under general anesthesia utilizing fluoroscopy.
Assess the posterior wall stability with the obturator oblique view. Hip will be in flexion, adduction and add axial load. Check the medial clear space for opening.
Irreducible isolated posterior dislocation
•Do emergency surgical treatment to reduce the hip.
Treatment of posterior hip dislocation with posterior acetabular wall fracture
•Must assess the stability of the hip joint by examination under anesthesia after closed reduction.
•After closed reduction, if the dislocation is not congruent, do open reduction and fixation urgently.
Treatment of Pipkin femoral head fractures
•Headless screw fixation.
Видео Dislocation of the hip - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
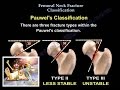 Femoral Neck Fracture Classification - Everything You Need To Know - Dr. Nabil Ebraheim
Femoral Neck Fracture Classification - Everything You Need To Know - Dr. Nabil Ebraheim Developmental Dysplasia of the Hip and the Pavlik Harness
Developmental Dysplasia of the Hip and the Pavlik Harness Hip Injuries | Hip Dislocation | Orthopedic Surgery Lectures | V-Learning | sqadia.com
Hip Injuries | Hip Dislocation | Orthopedic Surgery Lectures | V-Learning | sqadia.com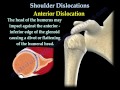 Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim
Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim Hip Examination - Orthopaedics
Hip Examination - Orthopaedics A Review Of Acetabular Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
A Review Of Acetabular Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Hip Dislocation
Hip Dislocation Ankle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Ankle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Knee Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim
Knee Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Understanding Hip Dysplasia | Boston Children's Hospital
Understanding Hip Dysplasia | Boston Children's Hospital Hip Labral Tear? Pain or Popping in Your Hip? Try This Exercise NOW!
Hip Labral Tear? Pain or Popping in Your Hip? Try This Exercise NOW!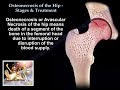 Osteonecrosis Of The Hip Stages & Treatment - Everything You Need To Know - Dr. Nabil
Osteonecrosis Of The Hip Stages & Treatment - Everything You Need To Know - Dr. Nabil How to POP Your Hip Back in Place
How to POP Your Hip Back in Place Extreme Hip Pain Gone INSTANTLY!
Extreme Hip Pain Gone INSTANTLY! Anatomy Of The Acetabulum - Everything You Need To Know - Dr. Nabil Ebraheim
Anatomy Of The Acetabulum - Everything You Need To Know - Dr. Nabil Ebraheim Intertrochanteric Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Intertrochanteric Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Monteggia Fractures In Children
Monteggia Fractures In Children How to Self Correct a High Hip in 30 SECONDS
How to Self Correct a High Hip in 30 SECONDS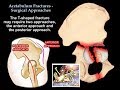 Acetabulum Fractures Surgical Approaches - Everything You Need To Know - Dr. Nabil Ebraheim
Acetabulum Fractures Surgical Approaches - Everything You Need To Know - Dr. Nabil Ebraheim