Subtrochanteric Femur Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes the subtrochanteric fractures, the etiology, signs and symptoms, diagnosis, and treatment options.
Subtrochanteric Femur Fractures are difficult fractures to manage and heal. The deforming forces and high stresses area across the fracture could lead to implant failure before union of the fracture. The subtrochanter area is defined as an area from the lesser trochanter to 5 cm distally. Subtrochanteric fractures occur within this area. May have intertrochanteric extension and is called a peritrochanteric fracture. It usually indicates a high energy trauma in young patient. it can occur in elderly from low energy trauma. Mortality rate of the elderly is about 25% within the first year. Try to exclude pathological fracture. Isolated fracture of the lesser trochanter may indicate a metastatic tumor. Try to exclude fracture caused by bisphosphonate alendronate. Bisphosphonate related fractures:
•Lateral cortical thickening
•Transverse fracture orientation
•Medial spike
•Lack of comminution.
Patient will complain of symptoms before the fracture occurs. Stop the bisphosphonate and give the patient anabolics that may prevent the fracture. If the patient is on bisphosphonate for 4 or more years and has pain get an x-ray. If you see cortical thickening get an MRI to rule out a stress fracture. Also check the vitamin D and calcium levels.
Unique aspects of the fracture
Transition from cancellous to cortical bone. The cortical bone vascularity and fracture surface area is less. There will also be high compressive forces medially and tensile forces laterally. The fracture may go to varus with fixation. Lateral plate acts as a tension band and is subject to bending load. Perfect reduction and medial cortex reconstitution in plating is very critical. Bone to bone transfer is important to avoid varus. Failure of the lateral plate is certain if early weight bearing is allowed. As little as 2 mm of separation of the medial cortex will lead to medial collapse and lateral plate bending failure. Strong muscle deforming forces in the proximal fragment. The distal fragment is also adducted and shortened by the adductor magnus muscle.
Classification
Usually divided into two types
1-No extension of the fracture into the piriformis fossa.
2-Extension into the greater trochanter with involvement of the piriformis fossa: elderly patients are more of this type.
Why is it important? The classification helps the surgeon to choose an appropriate device for fixation. Need to restore the medial buttress (bone to bone transfer) before the implant fails.
How to restore the medial buttress? By exact reduction of the medial fragment or by bone graft if there is a gap in the medial part of the fracture. The bone graft will consolidate and allow bone to bone transfer. The bone graft is usually used if there is an open fracture reduction and fixation technique or by chest tube if a closed technique is used. Bone healing by callus: weight bearing is used when there is x-ray evidence of healing.
How to treat Subtrochanteric Fractures? The Russel Taylor Classification is based on involvement of the lesser trochanter and the piriformis fossa. It provides guidance to the treatment of fractures with a nail, when nailing should be avoided and what type should be used such as a standard cephalomeduallry nail. Most Subtrochanteric Fractures are treated with IM rod especially if the fracture does not extend to the piriformis fossa or the greater trochanter.
Why choose a rod? Closed IM rod fixation is minimally invasive. IM rod preserves some vascularity. Stronger construct and load sharing. Positive effect on reaming that will give us bone graft. Insertion of the rod will not reduce the fracture, a small incision to reduce the fracture before reaming and inserting the rod is done if the fracture is not reduced. Piriformis fossa entry point is the gold standard and has the advantage of collinear trajectory with long access to the femoral shaft. It will avoid varus deformity. IM nail may be used in the elderly with a trochanteric entry point. Greater torchnateric entry may disrupt the abductor muscles.
Treatment:
•Intramedullary nail
•Proximal locking technique
•Proximal plate fixation with fixed angle device
•Nonunion of the Subtrochanter Fracture revision of the internal fixation selected bone graft.
•Some still use the compression hip screw.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Background music provided as a free download from YouTube Audio Library.
Song Title: Every Step
Видео Subtrochanteric Femur Fractures - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Subtrochanteric Femur Fractures are difficult fractures to manage and heal. The deforming forces and high stresses area across the fracture could lead to implant failure before union of the fracture. The subtrochanter area is defined as an area from the lesser trochanter to 5 cm distally. Subtrochanteric fractures occur within this area. May have intertrochanteric extension and is called a peritrochanteric fracture. It usually indicates a high energy trauma in young patient. it can occur in elderly from low energy trauma. Mortality rate of the elderly is about 25% within the first year. Try to exclude pathological fracture. Isolated fracture of the lesser trochanter may indicate a metastatic tumor. Try to exclude fracture caused by bisphosphonate alendronate. Bisphosphonate related fractures:
•Lateral cortical thickening
•Transverse fracture orientation
•Medial spike
•Lack of comminution.
Patient will complain of symptoms before the fracture occurs. Stop the bisphosphonate and give the patient anabolics that may prevent the fracture. If the patient is on bisphosphonate for 4 or more years and has pain get an x-ray. If you see cortical thickening get an MRI to rule out a stress fracture. Also check the vitamin D and calcium levels.
Unique aspects of the fracture
Transition from cancellous to cortical bone. The cortical bone vascularity and fracture surface area is less. There will also be high compressive forces medially and tensile forces laterally. The fracture may go to varus with fixation. Lateral plate acts as a tension band and is subject to bending load. Perfect reduction and medial cortex reconstitution in plating is very critical. Bone to bone transfer is important to avoid varus. Failure of the lateral plate is certain if early weight bearing is allowed. As little as 2 mm of separation of the medial cortex will lead to medial collapse and lateral plate bending failure. Strong muscle deforming forces in the proximal fragment. The distal fragment is also adducted and shortened by the adductor magnus muscle.
Classification
Usually divided into two types
1-No extension of the fracture into the piriformis fossa.
2-Extension into the greater trochanter with involvement of the piriformis fossa: elderly patients are more of this type.
Why is it important? The classification helps the surgeon to choose an appropriate device for fixation. Need to restore the medial buttress (bone to bone transfer) before the implant fails.
How to restore the medial buttress? By exact reduction of the medial fragment or by bone graft if there is a gap in the medial part of the fracture. The bone graft will consolidate and allow bone to bone transfer. The bone graft is usually used if there is an open fracture reduction and fixation technique or by chest tube if a closed technique is used. Bone healing by callus: weight bearing is used when there is x-ray evidence of healing.
How to treat Subtrochanteric Fractures? The Russel Taylor Classification is based on involvement of the lesser trochanter and the piriformis fossa. It provides guidance to the treatment of fractures with a nail, when nailing should be avoided and what type should be used such as a standard cephalomeduallry nail. Most Subtrochanteric Fractures are treated with IM rod especially if the fracture does not extend to the piriformis fossa or the greater trochanter.
Why choose a rod? Closed IM rod fixation is minimally invasive. IM rod preserves some vascularity. Stronger construct and load sharing. Positive effect on reaming that will give us bone graft. Insertion of the rod will not reduce the fracture, a small incision to reduce the fracture before reaming and inserting the rod is done if the fracture is not reduced. Piriformis fossa entry point is the gold standard and has the advantage of collinear trajectory with long access to the femoral shaft. It will avoid varus deformity. IM nail may be used in the elderly with a trochanteric entry point. Greater torchnateric entry may disrupt the abductor muscles.
Treatment:
•Intramedullary nail
•Proximal locking technique
•Proximal plate fixation with fixed angle device
•Nonunion of the Subtrochanter Fracture revision of the internal fixation selected bone graft.
•Some still use the compression hip screw.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Background music provided as a free download from YouTube Audio Library.
Song Title: Every Step
Видео Subtrochanteric Femur Fractures - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Intertrochanteric Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Intertrochanteric Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim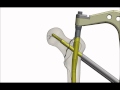 A-PFN (Antirotator Proksimal Femur Çivisi) (Antirotator Proximal Femoral Nail)
A-PFN (Antirotator Proksimal Femur Çivisi) (Antirotator Proximal Femoral Nail) Frozen Shoulder Adhesive Capsulitis - Everything You Need To Know - Dr. Nabil Ebraheim
Frozen Shoulder Adhesive Capsulitis - Everything You Need To Know - Dr. Nabil Ebraheim Nasty Subtrochanteric Femur Fractures
Nasty Subtrochanteric Femur Fractures Peritrochanteric Fractures- DHS Vs IM Nail
Peritrochanteric Fractures- DHS Vs IM Nail Piriformis Syndrome A Hidden Cause of Sciatica - Everything You Need To Know - Dr. Nabil Ebraheim
Piriformis Syndrome A Hidden Cause of Sciatica - Everything You Need To Know - Dr. Nabil Ebraheim Femur fracture ,Subtrochanteric fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Femur fracture ,Subtrochanteric fracture - Everything You Need To Know - Dr. Nabil Ebraheim Femoral Head Fracture Review, Pipken Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Femoral Head Fracture Review, Pipken Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Scaphoid Nonunion - Everything You Need To Know - Dr. Nabil Ebraheim
Scaphoid Nonunion - Everything You Need To Know - Dr. Nabil Ebraheim Hip Fractures, Types and fixation - Everything You Need To Know - Dr. Nabil Ebraheim
Hip Fractures, Types and fixation - Everything You Need To Know - Dr. Nabil Ebraheim Tibial Plateau Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Tibial Plateau Fractures - Everything You Need To Know - Dr. Nabil Ebraheim AO -pelvis both column fracture fixation through ilioinguinal pproach
AO -pelvis both column fracture fixation through ilioinguinal pproach Clavicle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Clavicle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim PF Gamma intramedullary nails system__Leon
PF Gamma intramedullary nails system__Leon Avoiding Complications Intertroch. Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Avoiding Complications Intertroch. Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim The Ideal Patient With Low Back Pain - Everything You Need To Know - Dr. Nabil Ebraheim
The Ideal Patient With Low Back Pain - Everything You Need To Know - Dr. Nabil Ebraheim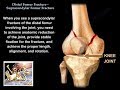 Distal Femur Supracondylar Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Distal Femur Supracondylar Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Fractures Of The Femur Shaft Winquist & Hansen - Everything You Need To Know - Dr. Nabil Ebraheim
Fractures Of The Femur Shaft Winquist & Hansen - Everything You Need To Know - Dr. Nabil Ebraheim DCS Locking Plate
DCS Locking Plate Bone Fractures Types Nursing Interventions, Treatment, Signs and Symptoms NCLEX
Bone Fractures Types Nursing Interventions, Treatment, Signs and Symptoms NCLEX