Femoral Head Fracture Review, Pipken Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes femoral head fractures - Pipken Classification.
Pipkin fractures usually occur with posterior dislocation of the hip. Posterior dislocation of the hip occurs in about 10% of cases. As the femoral head dislocates, it hits the posterior rim of the acetabulum and fractures. This is contrary to an anterior femoral head dislocation. Anterior dislocation will cause impaction fragment of the femoral head or indentation fractures. Pipkin fractures can also occur with anterior dislocations.
There are four fracture types within the pipkin fracture classification. These fracture types are a traumatic event that is characterized as dislocation and fracture of the femoral head. Remember, these fracture types range for least (Type I) to most severe (Type IV).
Type I: posterior dislocation with femoral head fracture caudad (inferior) to the fovea.
Type II: posterior dislocation with femoral head fracture cephalad (superior) to the fovea. Involves the weight bearing surface.
Type III: posterior dislocation with associated femoral neck fracture. Do open reduction of hip, neck and head. Do not do closed reduction (this may displace the neck fracture). Do ORIF of the head and neck through Watson-Jones approach or the Smith-Petersen approach.
Type IV: fracture of the femoral head associated with acetabulum fracture. Acetabulum fracture is posterior and the head fracture is anterior.
Some cases are associated with a dashboard injury. Try to examine the patient for injury to the posterior cruciate ligament (PCL). Both knees are flexed to 90° and the knee is viewed from the side to compare the positions of the anterior tibia. These examinations are helpful but may be difficult to perform when the patient is awake. Posterior drawer test is done with the patient in supine position and the knee is flexed to 90°. Examination for injury to the posterior cruciate ligament (PCL) can be done in the operating room when the patient is asleep or after fixing the acetabular fracture. These tests cannot be done in the emergency room! If you suspect a PCL injury, you may get an MRI.
Examine the sciatic nerve. Check for foot drop! Be aware that avascular necrosis may occur in these cases. Please advise the patient and family.
Treatment: Do a closed reduction of the hip within 6 hours unless you have a nondisplaced femoral neck fracture, then do open reduction of the neck and hip to avoid displacement of the femoral neck. After reduction of the hip, send the patient for x-rays and CT scans. Wait until after reduction of the hip due to the possible problem of avascular necrosis. Treat the patient according to this plan: if the patient has nondisplaced Type 1 fracture no surgery, especially if the hip is stable and there are no fragments within the hip joint. If the patient has a displaced pipkin fracture, need to do surgery especially if the patient has a pipkin type II fracture, femoral neck fracture or acetabular fracture. Some recommend surgery for a displaced pipkin type I fracture, do a Smith-Petersen approach.
The muscle interval is between two nerves. Smith Petersen approach: enter between the tenson fascia lata (superior gluteal nerve) and the Sartorius muscle (femoral nerve). Watch out for the lateral cutaneous nerve of the thigh.
The fracture can also be seen with an x-ray in surgery! Try to get the angle of the x-ray from information you find in the CT scan.
What is the angle of the fracture in the CT scan? CT scan angle at 30°. The x-ray in surgery will then be at 30°. Get the fracture in front of you by the x-ray. When placing the screws make sure you are not far off from the main fragment. Use compression screws that can be buried below the surface of the cartilage.
Sometimes a posterior approach to the hip is needed due to an acetabular fracture despite the fact that the femoral head fracture fragment is anterior. Posterior approach may be attempted, however if this is not successful, a trochanteric osteotomy may be added in order to visualize and fix the femoral head and acetabulum (Type IV pipkin)
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundation/home/Give_Online.aspx?sig=29
Видео Femoral Head Fracture Review, Pipken Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Pipkin fractures usually occur with posterior dislocation of the hip. Posterior dislocation of the hip occurs in about 10% of cases. As the femoral head dislocates, it hits the posterior rim of the acetabulum and fractures. This is contrary to an anterior femoral head dislocation. Anterior dislocation will cause impaction fragment of the femoral head or indentation fractures. Pipkin fractures can also occur with anterior dislocations.
There are four fracture types within the pipkin fracture classification. These fracture types are a traumatic event that is characterized as dislocation and fracture of the femoral head. Remember, these fracture types range for least (Type I) to most severe (Type IV).
Type I: posterior dislocation with femoral head fracture caudad (inferior) to the fovea.
Type II: posterior dislocation with femoral head fracture cephalad (superior) to the fovea. Involves the weight bearing surface.
Type III: posterior dislocation with associated femoral neck fracture. Do open reduction of hip, neck and head. Do not do closed reduction (this may displace the neck fracture). Do ORIF of the head and neck through Watson-Jones approach or the Smith-Petersen approach.
Type IV: fracture of the femoral head associated with acetabulum fracture. Acetabulum fracture is posterior and the head fracture is anterior.
Some cases are associated with a dashboard injury. Try to examine the patient for injury to the posterior cruciate ligament (PCL). Both knees are flexed to 90° and the knee is viewed from the side to compare the positions of the anterior tibia. These examinations are helpful but may be difficult to perform when the patient is awake. Posterior drawer test is done with the patient in supine position and the knee is flexed to 90°. Examination for injury to the posterior cruciate ligament (PCL) can be done in the operating room when the patient is asleep or after fixing the acetabular fracture. These tests cannot be done in the emergency room! If you suspect a PCL injury, you may get an MRI.
Examine the sciatic nerve. Check for foot drop! Be aware that avascular necrosis may occur in these cases. Please advise the patient and family.
Treatment: Do a closed reduction of the hip within 6 hours unless you have a nondisplaced femoral neck fracture, then do open reduction of the neck and hip to avoid displacement of the femoral neck. After reduction of the hip, send the patient for x-rays and CT scans. Wait until after reduction of the hip due to the possible problem of avascular necrosis. Treat the patient according to this plan: if the patient has nondisplaced Type 1 fracture no surgery, especially if the hip is stable and there are no fragments within the hip joint. If the patient has a displaced pipkin fracture, need to do surgery especially if the patient has a pipkin type II fracture, femoral neck fracture or acetabular fracture. Some recommend surgery for a displaced pipkin type I fracture, do a Smith-Petersen approach.
The muscle interval is between two nerves. Smith Petersen approach: enter between the tenson fascia lata (superior gluteal nerve) and the Sartorius muscle (femoral nerve). Watch out for the lateral cutaneous nerve of the thigh.
The fracture can also be seen with an x-ray in surgery! Try to get the angle of the x-ray from information you find in the CT scan.
What is the angle of the fracture in the CT scan? CT scan angle at 30°. The x-ray in surgery will then be at 30°. Get the fracture in front of you by the x-ray. When placing the screws make sure you are not far off from the main fragment. Use compression screws that can be buried below the surface of the cartilage.
Sometimes a posterior approach to the hip is needed due to an acetabular fracture despite the fact that the femoral head fracture fragment is anterior. Posterior approach may be attempted, however if this is not successful, a trochanteric osteotomy may be added in order to visualize and fix the femoral head and acetabulum (Type IV pipkin)
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundation/home/Give_Online.aspx?sig=29
Видео Femoral Head Fracture Review, Pipken Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim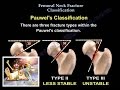 Femoral Neck Fracture Classification - Everything You Need To Know - Dr. Nabil Ebraheim
Femoral Neck Fracture Classification - Everything You Need To Know - Dr. Nabil Ebraheim Dislocation of the hip - Everything You Need To Know - Dr. Nabil Ebraheim
Dislocation of the hip - Everything You Need To Know - Dr. Nabil Ebraheim Blood Supply of Femoral Head | MADE EASY | NEET PG | Femur Anatomy - The Young Orthopod
Blood Supply of Femoral Head | MADE EASY | NEET PG | Femur Anatomy - The Young Orthopod Growth Plate Injuries , CHILDREN FRACTURES- Everything You Need To Know - Dr. Nabil Ebraheim
Growth Plate Injuries , CHILDREN FRACTURES- Everything You Need To Know - Dr. Nabil Ebraheim Hip Dislocations and Femoral Head Fractures
Hip Dislocations and Femoral Head Fractures Lisfranc Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
Lisfranc Injuries - Everything You Need To Know - Dr. Nabil Ebraheim Hip Replacement Surgery
Hip Replacement Surgery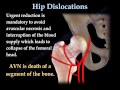 Hip Dislocations - Everything You Need To Know - Dr. Nabil Ebraheim
Hip Dislocations - Everything You Need To Know - Dr. Nabil Ebraheim Femoral Neck fracture Classifications - Everything You Need To Know - Dr. Nabil Ebraheim
Femoral Neck fracture Classifications - Everything You Need To Know - Dr. Nabil Ebraheim Avoiding Complications Intertroch. Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Avoiding Complications Intertroch. Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Basic Sciences - Blood Supply of the Femoral head
Basic Sciences - Blood Supply of the Femoral head Tibial Pilon Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Tibial Pilon Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Coronoid Process Fracture Treatment ,approaches Everything You Need To Know - Dr. Nabil Ebraheim
Coronoid Process Fracture Treatment ,approaches Everything You Need To Know - Dr. Nabil Ebraheim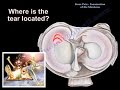 Knee Pain , Meniscus tear - Everything You Need To Know - Dr. Nabil Ebraheim
Knee Pain , Meniscus tear - Everything You Need To Know - Dr. Nabil Ebraheim Hip Fractures, Types and fixation - Everything You Need To Know - Dr. Nabil Ebraheim
Hip Fractures, Types and fixation - Everything You Need To Know - Dr. Nabil Ebraheim Ankle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Ankle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Pelvic Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Pelvic Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Femoral Neck Fractures Fixation - Everything You Need To Know - Dr. Nabil Ebraheim
Femoral Neck Fractures Fixation - Everything You Need To Know - Dr. Nabil Ebraheim Femoral neck fracture - applied anatomy
Femoral neck fracture - applied anatomy