Tibial Pilon Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes tibial pilon fractures.
High energy axial load injury. Soft tissue injury is bad. Closed or open fracture and ankle joint are usually involved. Metaphysis of the tibia is usually involved.
No immediate open reduction and internal fixation because soft tissue is usually bad. Early ORIF is not recommended. Initially, the treatment is usually closed reduction and a splint followed by staged ORIF.
In the operating room, start by applying external fixator. This decreases the incidence of wound complication and deep infection.
When internal fixation is used, it is better to use minimally invasive fixation.
Wait 1-3 weeks depending on the magnitude of the injury, the anticipated surgery and the presence of the wrinkle test.
After application of the external fixator, get a CT scan to check the joint and the fragments. This will help you to select the best operative approach in the future after the soft tissue condition improves. The physician needs to be aware that the AP radiographs may look OK, however, it may be misleading.
The joint usually has three fragments attached to ligaments. Because the ligaments are intact, the fragments can be pulled by the external fixator, which is called ligamentotaxis. The three fragments are:
1-Medial malleolus: attached to the deltoid ligament.
2-Anterolateral fragment: Chaput fragment (attached to the anterior inferior tibiofibular ligament). in children, this fragment is called Tillaux fracture. If the fracture involves avulsion of the fibula, it is called Wagstaffe fracture as rarely seen in some ankle fractures.
3-Volkmann fragment: posterolateral fragment attached to the posterior inferior tibiofibular ligament.
In this CT scan, you can see the three fragments of the pilon fracture as well as the joint impaction. When the fibula is intact, the lateral collateral ligament of the ankle may rupture (fibula is intact in 20% of the cases).
The break travel time in driving return to normal 6 weeks after initiation of weight bearing. In ankle fractures, it returns to normal 9 weeks after fixations (post-operatively).
The goal of surgery is anatomic reduction and stabilization of the articular surface. May start with fixation of the fibula with a plate or with a screw ( in some cases the screw is better because it is minimally invasive).
Fibular plate may add stability to the external fixator of the tibia, especially if there is a defect or comminution of the metaphysis of the tibia. Plating of the fibula adjunct to external fixation of the tibia. When there is a metaphyseal defect of the tibia, plating of the fibula can enhance the stiffness of the external fixator. Axial loading 2.2 times stiffer with plated fibula. Torsional force has no significant difference.
Approaches are many and it varies between limited approach and extensile approach. Try to protect the superficial peroneal nerve.
Dual incisions approach. Make sure that the distance between the incisions is no less than 7 cm. this is controversial.
Everybody agrees that staged ORIF is the best.
Significant disability in physical function was noted even with successful treatment in 36-item short form survey (SF-36).
Improvement of function and pain may take up to 2 years and eventually, about 10-15% may need arthrodesis.
Pilon fracture with a fracture of the tibial shaft:
Do fixation of the articular surface (usually percutaneously) then do fixation of the tibial shaft, usually with IM rodding.
Put external fixator calcaneal pins or talar pins. I usually put the calcaneal pin on the medial side of the ankle. Be aware of the location of the neurovascular structures, error in placement or the direction of the calcaneal pin can interfere with the neurovascular bundle. Avoid the bulge area. Application od the calcaneal traction pin is done at the posteromedial site. There is a ¾ distance between the palpable tip of the medial malleolus and the heel. The calcaneal transfixation pin is inserted in a transverse direction. It is better to keep the pin away from the area of future incisions.
Talus pin insertion
•Pin insertion should be medial to lateral.
•Anterodistal to anterior colliculus.
•Placement should be in 10 degrees anterocephalad direction.
Three principles of pilon fracture:
1-Anatomical reduction
2-Stable internal fixation
3-Early range of motion.
Achieving these three principles in every case of pilon fracture may not be possible.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Tibial Pilon Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
High energy axial load injury. Soft tissue injury is bad. Closed or open fracture and ankle joint are usually involved. Metaphysis of the tibia is usually involved.
No immediate open reduction and internal fixation because soft tissue is usually bad. Early ORIF is not recommended. Initially, the treatment is usually closed reduction and a splint followed by staged ORIF.
In the operating room, start by applying external fixator. This decreases the incidence of wound complication and deep infection.
When internal fixation is used, it is better to use minimally invasive fixation.
Wait 1-3 weeks depending on the magnitude of the injury, the anticipated surgery and the presence of the wrinkle test.
After application of the external fixator, get a CT scan to check the joint and the fragments. This will help you to select the best operative approach in the future after the soft tissue condition improves. The physician needs to be aware that the AP radiographs may look OK, however, it may be misleading.
The joint usually has three fragments attached to ligaments. Because the ligaments are intact, the fragments can be pulled by the external fixator, which is called ligamentotaxis. The three fragments are:
1-Medial malleolus: attached to the deltoid ligament.
2-Anterolateral fragment: Chaput fragment (attached to the anterior inferior tibiofibular ligament). in children, this fragment is called Tillaux fracture. If the fracture involves avulsion of the fibula, it is called Wagstaffe fracture as rarely seen in some ankle fractures.
3-Volkmann fragment: posterolateral fragment attached to the posterior inferior tibiofibular ligament.
In this CT scan, you can see the three fragments of the pilon fracture as well as the joint impaction. When the fibula is intact, the lateral collateral ligament of the ankle may rupture (fibula is intact in 20% of the cases).
The break travel time in driving return to normal 6 weeks after initiation of weight bearing. In ankle fractures, it returns to normal 9 weeks after fixations (post-operatively).
The goal of surgery is anatomic reduction and stabilization of the articular surface. May start with fixation of the fibula with a plate or with a screw ( in some cases the screw is better because it is minimally invasive).
Fibular plate may add stability to the external fixator of the tibia, especially if there is a defect or comminution of the metaphysis of the tibia. Plating of the fibula adjunct to external fixation of the tibia. When there is a metaphyseal defect of the tibia, plating of the fibula can enhance the stiffness of the external fixator. Axial loading 2.2 times stiffer with plated fibula. Torsional force has no significant difference.
Approaches are many and it varies between limited approach and extensile approach. Try to protect the superficial peroneal nerve.
Dual incisions approach. Make sure that the distance between the incisions is no less than 7 cm. this is controversial.
Everybody agrees that staged ORIF is the best.
Significant disability in physical function was noted even with successful treatment in 36-item short form survey (SF-36).
Improvement of function and pain may take up to 2 years and eventually, about 10-15% may need arthrodesis.
Pilon fracture with a fracture of the tibial shaft:
Do fixation of the articular surface (usually percutaneously) then do fixation of the tibial shaft, usually with IM rodding.
Put external fixator calcaneal pins or talar pins. I usually put the calcaneal pin on the medial side of the ankle. Be aware of the location of the neurovascular structures, error in placement or the direction of the calcaneal pin can interfere with the neurovascular bundle. Avoid the bulge area. Application od the calcaneal traction pin is done at the posteromedial site. There is a ¾ distance between the palpable tip of the medial malleolus and the heel. The calcaneal transfixation pin is inserted in a transverse direction. It is better to keep the pin away from the area of future incisions.
Talus pin insertion
•Pin insertion should be medial to lateral.
•Anterodistal to anterior colliculus.
•Placement should be in 10 degrees anterocephalad direction.
Three principles of pilon fracture:
1-Anatomical reduction
2-Stable internal fixation
3-Early range of motion.
Achieving these three principles in every case of pilon fracture may not be possible.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Tibial Pilon Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Foot Anatomy Animated Tutorial
Foot Anatomy Animated Tutorial Tibial Plafond Fracture Classification - Everything You Need To Know - Dr. Nabil Ebraheim
Tibial Plafond Fracture Classification - Everything You Need To Know - Dr. Nabil Ebraheim Monteggia Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Monteggia Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Lisfranc Injury - Everything You Need To Know - Dr. Nabil Ebraheim
Lisfranc Injury - Everything You Need To Know - Dr. Nabil Ebraheim Cauda Equina Syndrome - Everything You Need To Know - Dr. Nabil
Cauda Equina Syndrome - Everything You Need To Know - Dr. Nabil Supracondylar Fractures Of The Humerus In Children
Supracondylar Fractures Of The Humerus In Children Tibial Plateau Fracture Fixation, Proximal Tibia - Everything You Need To Know - Dr. Nabil Ebraheim
Tibial Plateau Fracture Fixation, Proximal Tibia - Everything You Need To Know - Dr. Nabil Ebraheim Ankle Pain Complete Overview - Everything You Need To Know - Dr. Nabil Ebraheim
Ankle Pain Complete Overview - Everything You Need To Know - Dr. Nabil Ebraheim Syndesmotic Injuries Of The Ankle - Everything You Need To Know - Dr. Nabil Ebraheim
Syndesmotic Injuries Of The Ankle - Everything You Need To Know - Dr. Nabil Ebraheim Tibial pilon fracture LCP distal tibial plate
Tibial pilon fracture LCP distal tibial plate Principles of Fracture Fixation | Orthopedic Basics
Principles of Fracture Fixation | Orthopedic Basics Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Common Types Of Distal Radius Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Intertrochanteric Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Intertrochanteric Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim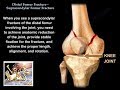 Distal Femur Supracondylar Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Distal Femur Supracondylar Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Ankle fracture / Fractures and its repair- Everything You Need To Know - Dr. Nabil Ebraheim
Ankle fracture / Fractures and its repair- Everything You Need To Know - Dr. Nabil Ebraheim Calcaneal Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Calcaneal Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Foot and Ankle Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
Foot and Ankle Injuries - Everything You Need To Know - Dr. Nabil Ebraheim Tibial Plateau Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Tibial Plateau Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Fracture Healing - Everything You Need To Know - Dr. Nabil Ebraheim
Fracture Healing - Everything You Need To Know - Dr. Nabil Ebraheim Pelvic Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Pelvic Fractures - Everything You Need To Know - Dr. Nabil Ebraheim