Jefferson Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes fractures types of the C1 cervical spine vertebrae, also called: Jefferson Fracture.
50% of patients will have associated spine injuries. The canal is wide with low risk of spinal cord injury unless the transverse ligament is disrupted. Difficult visualization on x-ray (usually see on the lateral side).
The junctional fracture could be missed.
The classic Jefferson fracture is a burst fracture that results from axial load. It could be a four-part fracture with bilateral fracture of the anterior and posterior arch.
There are variations which include two and three-part fractures. Incomplete formation of the posterior arch can be mistaken as a fracture.
Anatomy
C1 and C2 are stabilized together by the transverse ligament. C1 and C2 provide 50% of rotation of the neck. At the upper cervical region, the spinal canal is 2.5 times larger than the cord size. The stability and treatment of Jefferson fractures depend on the integrity of the transverse ligament and the displacement of the fracture.
You need to know the important ligaments related to the Jefferson fracture. C1 atlas fracture is axial load burst fracture. Is it just a bony injury or is it a bony and ligamentous injury.
Diagnosing ligamentous injury
A.D.I (atlanto dens interval) normally should be less than 3 mm in adults and less than 5 mm In children. If the A.D.I is between 3-5 mm, this means there is an injury to the transverse ligament ( the transverse ligament hold the odontoid and C1 together, alar and apical ligaments will be intact). More than 5 mm A.D.I, then there will be injury to the transverse alar and apical ligaments.
Fracture types
•Bony injury with intact transverse ligament. treatment depends on the type of injury to the transverse ligament. bony avulsion of the transverse ligament uses a halo cautiously. However some surgeons prefer to do fusion of C1 and C2.
•Lateral mass displacement less than 7 mm.
•Stable fracture: Treatment: Nondisplaced: rigid orthosis, displaced: use halo.
•In substance tear of the transverse ligament: treatment is C1-C2 fusion. Nee to do early surgery. Significant injury with risk of spinal cord compression.
Open mouth view
•Bony injury Jefferson fracture less than7 mm combined overhang, intact transverse ligament, stable fracture
•Jefferson fracture with more than 7 mm, combined overhang, torn transverse ligament, unstable fracture.
Radiological studies
CT scan is probably the best study in diagnosing the characteristics of bony injury. MRI is the best study in diagnosing any associated transverse ligament injury.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Jefferson Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
50% of patients will have associated spine injuries. The canal is wide with low risk of spinal cord injury unless the transverse ligament is disrupted. Difficult visualization on x-ray (usually see on the lateral side).
The junctional fracture could be missed.
The classic Jefferson fracture is a burst fracture that results from axial load. It could be a four-part fracture with bilateral fracture of the anterior and posterior arch.
There are variations which include two and three-part fractures. Incomplete formation of the posterior arch can be mistaken as a fracture.
Anatomy
C1 and C2 are stabilized together by the transverse ligament. C1 and C2 provide 50% of rotation of the neck. At the upper cervical region, the spinal canal is 2.5 times larger than the cord size. The stability and treatment of Jefferson fractures depend on the integrity of the transverse ligament and the displacement of the fracture.
You need to know the important ligaments related to the Jefferson fracture. C1 atlas fracture is axial load burst fracture. Is it just a bony injury or is it a bony and ligamentous injury.
Diagnosing ligamentous injury
A.D.I (atlanto dens interval) normally should be less than 3 mm in adults and less than 5 mm In children. If the A.D.I is between 3-5 mm, this means there is an injury to the transverse ligament ( the transverse ligament hold the odontoid and C1 together, alar and apical ligaments will be intact). More than 5 mm A.D.I, then there will be injury to the transverse alar and apical ligaments.
Fracture types
•Bony injury with intact transverse ligament. treatment depends on the type of injury to the transverse ligament. bony avulsion of the transverse ligament uses a halo cautiously. However some surgeons prefer to do fusion of C1 and C2.
•Lateral mass displacement less than 7 mm.
•Stable fracture: Treatment: Nondisplaced: rigid orthosis, displaced: use halo.
•In substance tear of the transverse ligament: treatment is C1-C2 fusion. Nee to do early surgery. Significant injury with risk of spinal cord compression.
Open mouth view
•Bony injury Jefferson fracture less than7 mm combined overhang, intact transverse ligament, stable fracture
•Jefferson fracture with more than 7 mm, combined overhang, torn transverse ligament, unstable fracture.
Radiological studies
CT scan is probably the best study in diagnosing the characteristics of bony injury. MRI is the best study in diagnosing any associated transverse ligament injury.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Jefferson Fracture - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Cervical Spine Trauma - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Spine Trauma - Everything You Need To Know - Dr. Nabil Ebraheim Hangman's Fracture, C2 Fracture - Everything You Need To Know - Dr. Nabil Ebraheim
Hangman's Fracture, C2 Fracture - Everything You Need To Know - Dr. Nabil Ebraheim Jefferson fracture - radiology video tutorial (x-ray, CT)
Jefferson fracture - radiology video tutorial (x-ray, CT)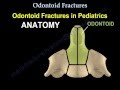 Odontoid Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Odontoid Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Common Problems Affecting The Biceps - Everything You Need To Know - Dr. Nabil Ebraheim
Common Problems Affecting The Biceps - Everything You Need To Know - Dr. Nabil Ebraheim Fracture Of The Radial Head Essex Lopresti - Everything You Need To Know - Dr. Nabil Ebraheim
Fracture Of The Radial Head Essex Lopresti - Everything You Need To Know - Dr. Nabil Ebraheim Compression vs. Burst Fractures
Compression vs. Burst Fractures Cervical Spine Myelopathy - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Spine Myelopathy - Everything You Need To Know - Dr. Nabil Ebraheim Ankle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Ankle Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Stress Fractures Of The Metatarsal Bones - Everything You Need To Know - Dr. Nabil Ebraheim
Stress Fractures Of The Metatarsal Bones - Everything You Need To Know - Dr. Nabil Ebraheim Spondylolysis,Spondylolisthesis,Spondylitis&Spondylosis-EverythingYou Need To Know-Dr.Nabil Ebraheim
Spondylolysis,Spondylolisthesis,Spondylitis&Spondylosis-EverythingYou Need To Know-Dr.Nabil Ebraheim Cervical Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim General Trauma Management,the injured patient- Everything You Need To Know - Dr. Nabil Ebraheim
General Trauma Management,the injured patient- Everything You Need To Know - Dr. Nabil Ebraheim Lumbar Spinal Stenosis - Everything You Need To Know - Dr. Nabil Ebraheim
Lumbar Spinal Stenosis - Everything You Need To Know - Dr. Nabil Ebraheim C1 and C2 Atlantoaxial Instability
C1 and C2 Atlantoaxial Instability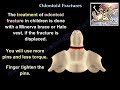 Odontoid Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Odontoid Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Odontoid Fractures in the Adult Population by Andrew Dailey, MD
Odontoid Fractures in the Adult Population by Andrew Dailey, MD Spinal Trauma: Cervical Trauma Protocol, Common Spinal Fractures – Radiology | Lecturio
Spinal Trauma: Cervical Trauma Protocol, Common Spinal Fractures – Radiology | Lecturio Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim
Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Hip Fractures - Everything You Need To Know - Dr. Nabil Ebraheim