Cervical Spine Myelopathy - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes the condition of Cervical Spine Myelopathy.
Myelopathy can occur due to compression of the cervical spinal cord. Pain is usually absent or poorly defined with vague sensory and motor changes
Signs and symptoms
•Wide slow broad-based ataxic gait pattern.
•Poor hand fine motor function and dexterity occurs early (writing, unable to hold a coffee cup or button a shirt).
•Myelopathic hand syndrome
•Thenar atrophy
positive grip and release sign, patient is unable to make a fist and release 20 times in 10 seconds.
•Positive finger escape sign: when the patient keeps the fingers extended, the ulnar digit tends to abduct.
•Pathological long tract signs will be seen consisting of Hoffman's, Babinski, clonus, finger escape and L’hermitte’s signs, in addition to hyperreflexia.
•Hoffman’s sign: flicking the nail of the middle or ring finger to produce flexion of the index finger to the thumb.
•Babinski: running a sharp instrument along the lateral border of the foot from the calcaneus produces extension of the big toe and fanning of the other toes.
•Clonus sign: nonvoluntary sustained movement of the ankle muscles with from passive continuous stretch.
•L’hermitte’s sign: neck flexion causing electric shock sensation and paresthesia radiating into the upper and lower extremity.
•Lower extremity dysfunction and spasticity.
•Bowel and bladder involvement is late.
Causes
•Cervical spondylothesis
•OPLL in Asians
•Tumor
•Congenital stenosis of the cervical spine canal
•Herniated disc.
Differential diagnosis
•Syringiomyelia
•Spinal cord tumor
•Multiple sclerosis: will have cranial nerve involvement. The jaw jerk test is positive.
•Amyotrphic lateral sclerosis (ALS): affects both iupper and lower extremities with no sensory changes.
Nurick classification
•Deals with walking ability and gait.
•Ranges from normal to wheel chair bound (in training exam).
MRI is the best study: it shows the compression and the changes in the spinal cord (bright signal in T2).
Prognosis:
•The condition does not improve without surgery.
•It tends to be progressive and gets worse in a steplike deterioration fashion with periods of stable symptoms (in-training exam).
•Decompression and fusion in case the symptoms are progressive or severe.
•Prognosis for recovery is better in patients with early surgery.
Surgery is usually done anteriorly with decompression and fusion.
Surgery is usually done with anterior cervical discectomy and fusion (ACDF).
Decompression
Bone graft for fusion
Plate&screws
In patient with low back pain and gait disturbance, look into the spinal cord, especially into the cervical spine. Don’t focus on the lumbar region, get a cervical spine MRI.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Cervical Spine Myelopathy - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Myelopathy can occur due to compression of the cervical spinal cord. Pain is usually absent or poorly defined with vague sensory and motor changes
Signs and symptoms
•Wide slow broad-based ataxic gait pattern.
•Poor hand fine motor function and dexterity occurs early (writing, unable to hold a coffee cup or button a shirt).
•Myelopathic hand syndrome
•Thenar atrophy
positive grip and release sign, patient is unable to make a fist and release 20 times in 10 seconds.
•Positive finger escape sign: when the patient keeps the fingers extended, the ulnar digit tends to abduct.
•Pathological long tract signs will be seen consisting of Hoffman's, Babinski, clonus, finger escape and L’hermitte’s signs, in addition to hyperreflexia.
•Hoffman’s sign: flicking the nail of the middle or ring finger to produce flexion of the index finger to the thumb.
•Babinski: running a sharp instrument along the lateral border of the foot from the calcaneus produces extension of the big toe and fanning of the other toes.
•Clonus sign: nonvoluntary sustained movement of the ankle muscles with from passive continuous stretch.
•L’hermitte’s sign: neck flexion causing electric shock sensation and paresthesia radiating into the upper and lower extremity.
•Lower extremity dysfunction and spasticity.
•Bowel and bladder involvement is late.
Causes
•Cervical spondylothesis
•OPLL in Asians
•Tumor
•Congenital stenosis of the cervical spine canal
•Herniated disc.
Differential diagnosis
•Syringiomyelia
•Spinal cord tumor
•Multiple sclerosis: will have cranial nerve involvement. The jaw jerk test is positive.
•Amyotrphic lateral sclerosis (ALS): affects both iupper and lower extremities with no sensory changes.
Nurick classification
•Deals with walking ability and gait.
•Ranges from normal to wheel chair bound (in training exam).
MRI is the best study: it shows the compression and the changes in the spinal cord (bright signal in T2).
Prognosis:
•The condition does not improve without surgery.
•It tends to be progressive and gets worse in a steplike deterioration fashion with periods of stable symptoms (in-training exam).
•Decompression and fusion in case the symptoms are progressive or severe.
•Prognosis for recovery is better in patients with early surgery.
Surgery is usually done anteriorly with decompression and fusion.
Surgery is usually done with anterior cervical discectomy and fusion (ACDF).
Decompression
Bone graft for fusion
Plate&screws
In patient with low back pain and gait disturbance, look into the spinal cord, especially into the cervical spine. Don’t focus on the lumbar region, get a cervical spine MRI.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Cervical Spine Myelopathy - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 What is Cervical Stenosis? | Jeffrey Cantor, MD
What is Cervical Stenosis? | Jeffrey Cantor, MD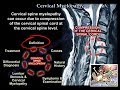 Cervical Myelopathy - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Myelopathy - Everything You Need To Know - Dr. Nabil Ebraheim $650K Result: Animated C4-7 Anterior Cervical Discectomy with Fusion
$650K Result: Animated C4-7 Anterior Cervical Discectomy with Fusion Cervical Myelopathy - What is it? How can we treat it?
Cervical Myelopathy - What is it? How can we treat it? Cervical Myelopathy | Spinal Cord Compression | Dr. Jason Koreckij of Columbia Orthopaedic Group
Cervical Myelopathy | Spinal Cord Compression | Dr. Jason Koreckij of Columbia Orthopaedic Group Cervical Spine Nerve Root Exam - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Spine Nerve Root Exam - Everything You Need To Know - Dr. Nabil Ebraheim Noncontrast MRI cervical spine search pattern
Noncontrast MRI cervical spine search pattern Cervical Spondylotic Myelopathy Cluster
Cervical Spondylotic Myelopathy Cluster How to Read a Spine MRI
How to Read a Spine MRI C3 C4 C5 Definitions. Cervical Spinal Cord Injury Symptoms, Causes, Treatments, and Recovery.
C3 C4 C5 Definitions. Cervical Spinal Cord Injury Symptoms, Causes, Treatments, and Recovery. Cervical Spinal Stenosis | Q&A with Dr. Brian J. Neuman
Cervical Spinal Stenosis | Q&A with Dr. Brian J. Neuman Syndrome: Myelopathy
Syndrome: Myelopathy Myelopathy vs Radiculopathy - Great Review!
Myelopathy vs Radiculopathy - Great Review! Myelopathy
Myelopathy Management of Cervical Stenosis: Anterior vs Posterior Approaches by Charles Sansur, M.D.
Management of Cervical Stenosis: Anterior vs Posterior Approaches by Charles Sansur, M.D. Neck Pain, Cervical Disc Herniation & Radiculopathy-Everything You Need To Know - Dr. Nabil Ebraheim
Neck Pain, Cervical Disc Herniation & Radiculopathy-Everything You Need To Know - Dr. Nabil Ebraheim Cervical Spine Myelopathy & Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Spine Myelopathy & Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim Cervical Myelopathy - Dr. Adewale Adeniran
Cervical Myelopathy - Dr. Adewale Adeniran Cervical Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim How to Read a MRI of Cervical Stenosis with Spinal Cord Injury | Spine Surgeon in Colorado
How to Read a MRI of Cervical Stenosis with Spinal Cord Injury | Spine Surgeon in Colorado