Spine tumors 6 – Cysts and Summary
Spine tumors 6 – Cysts and Summary
A few lesions within the spinal canal are predominantly cystic or nonenhancing. They are almost always intradural extramedullary. The three most common entities are arachnoid cysts, dermoid cysts, and neuroenteric cysts. A contrast enhanced myelogram can often give you a little bit more information about what the entity is by determining if it fills with contrast.
0:59 Case 1. Arachnoid cyst. Arachnoid cysts in the spine are somewhat uncommon but will have the same characteristics as CSF on all images. They may often be identified only by their deflection of the spinal cord and mass effect. Their main differential is arachnoid webs or adhesions which cause similar mass effect on the spinal cord. On myelography, they often fill with contrast but more slowly than the surrounding CSF.
3:37 Case 2. Dermoid. Dermal inclusion cysts, or dermoids, are complex lesions made out of tissue from more than one embryonal layer. Their characteristic feature is internal fat contents. Like intracranial dermoids, they can rupture and cause a chemical meningitis. Their appearance overlaps with lipomas but they are more likely to have complex features
5:02 Case 3. Neuroenteric cysts. Neuroenteric cysts are relatively simple cystic lesions which often occur ventral to the brainstem or spinal cord. They often are similar to but not exactly like CSF, and can be T1 hyperintense. They are indolent lesions but can cause mass effect. They do not fill on myelography.
6:57 Cyst summary. These are three of the most common cystic lesions. They are best differentiated by whether they communicate with the thecal sac (arachoid cysts), have complex or fatty features (dermoids), or are ventral to the cord and slightly differ from CSF (neuroenteric cysts).
7:36 Summary of spine tumors by location. Overall, when thinking about spine tumor, you should take a location-based approach. If you haven’t seen the introduction video yet, then definitely check it out. When divided by intramedullary, intradural extramedullary, and extradural, this can help you decide what type of lesion you are dealing with. Overall, always remember that the spine is an extension of the central nervous system, and consider imaging the brain because that may help you hone your differential diagnosis.
If you don't already, be sure to follow me on Twitter for more great updates:
https://twitter.com/BrentWeinberg
Check out this video and additional content on http://www.learnneuroradiology.com
Видео Spine tumors 6 – Cysts and Summary канала LearnNeuroradiology
A few lesions within the spinal canal are predominantly cystic or nonenhancing. They are almost always intradural extramedullary. The three most common entities are arachnoid cysts, dermoid cysts, and neuroenteric cysts. A contrast enhanced myelogram can often give you a little bit more information about what the entity is by determining if it fills with contrast.
0:59 Case 1. Arachnoid cyst. Arachnoid cysts in the spine are somewhat uncommon but will have the same characteristics as CSF on all images. They may often be identified only by their deflection of the spinal cord and mass effect. Their main differential is arachnoid webs or adhesions which cause similar mass effect on the spinal cord. On myelography, they often fill with contrast but more slowly than the surrounding CSF.
3:37 Case 2. Dermoid. Dermal inclusion cysts, or dermoids, are complex lesions made out of tissue from more than one embryonal layer. Their characteristic feature is internal fat contents. Like intracranial dermoids, they can rupture and cause a chemical meningitis. Their appearance overlaps with lipomas but they are more likely to have complex features
5:02 Case 3. Neuroenteric cysts. Neuroenteric cysts are relatively simple cystic lesions which often occur ventral to the brainstem or spinal cord. They often are similar to but not exactly like CSF, and can be T1 hyperintense. They are indolent lesions but can cause mass effect. They do not fill on myelography.
6:57 Cyst summary. These are three of the most common cystic lesions. They are best differentiated by whether they communicate with the thecal sac (arachoid cysts), have complex or fatty features (dermoids), or are ventral to the cord and slightly differ from CSF (neuroenteric cysts).
7:36 Summary of spine tumors by location. Overall, when thinking about spine tumor, you should take a location-based approach. If you haven’t seen the introduction video yet, then definitely check it out. When divided by intramedullary, intradural extramedullary, and extradural, this can help you decide what type of lesion you are dealing with. Overall, always remember that the spine is an extension of the central nervous system, and consider imaging the brain because that may help you hone your differential diagnosis.
If you don't already, be sure to follow me on Twitter for more great updates:
https://twitter.com/BrentWeinberg
Check out this video and additional content on http://www.learnneuroradiology.com
Видео Spine tumors 6 – Cysts and Summary канала LearnNeuroradiology
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Neuroradiology spine lesions - Case 1 - aggressive choice - Choose your own adventure
Neuroradiology spine lesions - Case 1 - aggressive choice - Choose your own adventure Fast 10: Neuroradiology high speed case review part 6 - Cases 51-60
Fast 10: Neuroradiology high speed case review part 6 - Cases 51-60 Neuroradiology board review lecture 1 case 8
Neuroradiology board review lecture 1 case 8 Basic neuroradiology procedures part 3 - Myelogram
Basic neuroradiology procedures part 3 - Myelogram Vascular Imaging of the Head and Neck - Case C
Vascular Imaging of the Head and Neck - Case C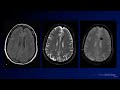 Neuroradiology Board Review - Brain Tumors - Case 12
Neuroradiology Board Review - Brain Tumors - Case 12 Neuroradiology spine lesions - Case 1 - nonaggressive choice - Choose your own adventure
Neuroradiology spine lesions - Case 1 - nonaggressive choice - Choose your own adventure Neuroradiology spine lesions - Case 2 - overview - Choose your own adventure
Neuroradiology spine lesions - Case 2 - overview - Choose your own adventure Nasopharyngeal Cancer Staging in 5 minutes
Nasopharyngeal Cancer Staging in 5 minutes Neuroradiology board review 3 case 1
Neuroradiology board review 3 case 1 Neuroradiology board review 3 case 17
Neuroradiology board review 3 case 17 Neuroradiology spine lesions - Case 4 - aggressive choice - Choose your own adventure
Neuroradiology spine lesions - Case 4 - aggressive choice - Choose your own adventure Neuroradiology board review 2 case 10
Neuroradiology board review 2 case 10 Neuroradiology board review lecture 1 case 15
Neuroradiology board review lecture 1 case 15 Basic Neuroradiology - Chapter 7 - Satisfaction of Search
Basic Neuroradiology - Chapter 7 - Satisfaction of Search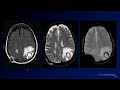 Neuroradiology Board Review - Brain Tumors - Case 3
Neuroradiology Board Review - Brain Tumors - Case 3 Neuroradiology board review 3 case 12
Neuroradiology board review 3 case 12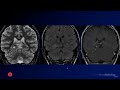 Neuroradiology Board Review - Brain Tumors - Case 16
Neuroradiology Board Review - Brain Tumors - Case 16 Fast 10: Neuroradiology high speed case review part 4 - Cases 31-40
Fast 10: Neuroradiology high speed case review part 4 - Cases 31-40 Neuroradiology board review 3 case 11
Neuroradiology board review 3 case 11 Neuroradiology spine lesions - Choose your own adventure - Introduction
Neuroradiology spine lesions - Choose your own adventure - Introduction