Giant Cell Tumor - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes the condition of Giant Cell Tumor.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
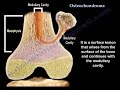
A giant cell tumor is a benign, locally aggressive tumor with bone destruction and with malignant potential. Giant cell tumors occur more in females and usually occur in skeletally mature patients. Giant cell tumors occur more in the distal femur, but they can occur in the proximal tibia, distal radius, proximal humerus, hand, spine (vertebral body), and the sacrum. When a giant cell tumor occurs in the sacrum, it occurs in the Ala, which is different from chordomas which occur in the midline of the sacrum. A giant cell tumor is an eccentric lesion that is lytic or radiolucent, and lies within the epiphysis/metaphysis area of the bone.
Plain x-rays are usually diagnostic and the lesion is usually geographic. This rumor rarely extends to the articular cartilage; however, it can break through the cortex into the surrounding tissues. Pulmonary metastases occur in about 2% and theses lesions are usually benign. Get chest x-rays or Ct scans of the chest as part of the diagnostic workup.
In pathology, the giant cell tumor contains large multinucleated giant cells in addition to mononuclear stromal cells. The stroma cells look like the nuclei of the giant cells. The mononuclear stromal cells are the neoplastic cells. The giant cells are similar to osteoclasts and are directed through RANKL pathways to cause bone destruction. The tumor may have secondary Aneurysmal Bone Cyst (ABC) component.
The physician should rule out hyperparathyroidism or Brown Tumor. With multiple lesions (multiple giant cells) and in hyperparathyroidism, the serum calcium level is high. Giant cell tumors can appear in other pathological conditions, such as aneurysmal bone cysts, fractures, and chondroblastomas. If you see giant cells under the microscope, this does not mean that the patient has a giant cell tumor. Epiphyseal tumors such as chondroblastoma (young patients) and clear-cell chondrosarcoma (adult patients) should be ruled out as well. In the sacrum, you need to differentiate a Giant Cell Tumor from Chordoma. Chordoma will have a central location.
Primary malignant giant cell tumors have a greater chance of metastasis. This tumor behaves like an osteosarcoma with an abundance of giant cells (it is a different type of tumor). Metastasis can occur in about 5% of cases. Secondary malignant giant cell tumors can occur following radiation or following unsuccessful attempts at removal of the giant cell tumor with recurrence. When there is recurrence of the tumor, you will see the radiolucent zone and then biopsy the tumor again.
Medical treatment consists of bisphosphonate and denosumab (will act on the RANK pathway). Denosumab is a human monoclonal antibody that is used in recurrent disease and when wide resection may cause significant morbidity. Denosumab is used in unresectable Giant Cell Tumors or when there is recurrence, or when the tumor is aggressive. Aggressive curettage and the use of the adjuvant (can be phenol, hydrogen peroxide, or cryotherapy). The adjuvant decreases the microscopic disease and reduces the recurrence. After the aggressive curettage, the defect can be filled with bone graft or cement, plus or minus fixation. Resection and reconstruction is usually done in aggressive lesion if the tumor erodes or extends to the soft tissues, or in recurrent cases. Resection and reconstruction can also be done when there is involvement of the subchondral bone.
Видео Giant Cell Tumor - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
A giant cell tumor is a benign, locally aggressive tumor with bone destruction and with malignant potential. Giant cell tumors occur more in females and usually occur in skeletally mature patients. Giant cell tumors occur more in the distal femur, but they can occur in the proximal tibia, distal radius, proximal humerus, hand, spine (vertebral body), and the sacrum. When a giant cell tumor occurs in the sacrum, it occurs in the Ala, which is different from chordomas which occur in the midline of the sacrum. A giant cell tumor is an eccentric lesion that is lytic or radiolucent, and lies within the epiphysis/metaphysis area of the bone.
Plain x-rays are usually diagnostic and the lesion is usually geographic. This rumor rarely extends to the articular cartilage; however, it can break through the cortex into the surrounding tissues. Pulmonary metastases occur in about 2% and theses lesions are usually benign. Get chest x-rays or Ct scans of the chest as part of the diagnostic workup.
In pathology, the giant cell tumor contains large multinucleated giant cells in addition to mononuclear stromal cells. The stroma cells look like the nuclei of the giant cells. The mononuclear stromal cells are the neoplastic cells. The giant cells are similar to osteoclasts and are directed through RANKL pathways to cause bone destruction. The tumor may have secondary Aneurysmal Bone Cyst (ABC) component.
The physician should rule out hyperparathyroidism or Brown Tumor. With multiple lesions (multiple giant cells) and in hyperparathyroidism, the serum calcium level is high. Giant cell tumors can appear in other pathological conditions, such as aneurysmal bone cysts, fractures, and chondroblastomas. If you see giant cells under the microscope, this does not mean that the patient has a giant cell tumor. Epiphyseal tumors such as chondroblastoma (young patients) and clear-cell chondrosarcoma (adult patients) should be ruled out as well. In the sacrum, you need to differentiate a Giant Cell Tumor from Chordoma. Chordoma will have a central location.
Primary malignant giant cell tumors have a greater chance of metastasis. This tumor behaves like an osteosarcoma with an abundance of giant cells (it is a different type of tumor). Metastasis can occur in about 5% of cases. Secondary malignant giant cell tumors can occur following radiation or following unsuccessful attempts at removal of the giant cell tumor with recurrence. When there is recurrence of the tumor, you will see the radiolucent zone and then biopsy the tumor again.
Medical treatment consists of bisphosphonate and denosumab (will act on the RANK pathway). Denosumab is a human monoclonal antibody that is used in recurrent disease and when wide resection may cause significant morbidity. Denosumab is used in unresectable Giant Cell Tumors or when there is recurrence, or when the tumor is aggressive. Aggressive curettage and the use of the adjuvant (can be phenol, hydrogen peroxide, or cryotherapy). The adjuvant decreases the microscopic disease and reduces the recurrence. After the aggressive curettage, the defect can be filled with bone graft or cement, plus or minus fixation. Resection and reconstruction is usually done in aggressive lesion if the tumor erodes or extends to the soft tissues, or in recurrent cases. Resection and reconstruction can also be done when there is involvement of the subchondral bone.
Видео Giant Cell Tumor - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Osteochondroma , solitary and multiple . Everything You Need To Know - Dr. Nabil Ebraheim
Osteochondroma , solitary and multiple . Everything You Need To Know - Dr. Nabil Ebraheim Giant Cell Tumor: Morphology, Pathogenesis
Giant Cell Tumor: Morphology, Pathogenesis Mallet Finger Complete - Everything You Need To Know - Dr. Nabil Ebraheim
Mallet Finger Complete - Everything You Need To Know - Dr. Nabil Ebraheim Bone Lesions: Radiographic Assessment, Part 1, by Geoffrey Riley, MD
Bone Lesions: Radiographic Assessment, Part 1, by Geoffrey Riley, MD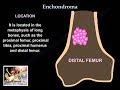 Enchondroma - Everything You Need To Know - Dr. Nabil Ebraheim
Enchondroma - Everything You Need To Know - Dr. Nabil Ebraheim Bone tumors - causes, symptoms, diagnosis, treatment, pathology
Bone tumors - causes, symptoms, diagnosis, treatment, pathology Biceps Brachii Anatomy - Everything You Need To Know - Dr. Nabil Ebraheim
Biceps Brachii Anatomy - Everything You Need To Know - Dr. Nabil Ebraheim Osteomyelitis Bone Infection - Everything You Need To Know - Dr. Nabil Ebraheim
Osteomyelitis Bone Infection - Everything You Need To Know - Dr. Nabil Ebraheim Giant Cell Tumor VS Aneurysmal Bone cyst || GCT VS ABC || Xrays || Image bases || Radiology ||
Giant Cell Tumor VS Aneurysmal Bone cyst || GCT VS ABC || Xrays || Image bases || Radiology || GIANT CELL TUMOUR I GCT (Bone Tumour) - Causes I Symptoms I Treatment I Surgery by Dr Rajat Gupta
GIANT CELL TUMOUR I GCT (Bone Tumour) - Causes I Symptoms I Treatment I Surgery by Dr Rajat Gupta Malignant Bone Tumors | USMLE COMLEX NCLEX
Malignant Bone Tumors | USMLE COMLEX NCLEX Arthritis Of The Fingers - Everything You Need To Know - Dr. Nabil Ebraheim
Arthritis Of The Fingers - Everything You Need To Know - Dr. Nabil Ebraheim Bone and cartilage tumors
Bone and cartilage tumors Fibrous Dysplasia - Everything You Need To Know - Dr. Nabil Ebraheim
Fibrous Dysplasia - Everything You Need To Know - Dr. Nabil Ebraheim GCT & PVNS (Giant Cell Tumor of Tendon Sheath & Pigmented Villonodular Synovitis)
GCT & PVNS (Giant Cell Tumor of Tendon Sheath & Pigmented Villonodular Synovitis) Patellar Fractures - Everything You Need To Know - Dr. Nabil Ebraheim
Patellar Fractures - Everything You Need To Know - Dr. Nabil Ebraheim Osteoid Osteoma - Everything You Need To Know - Dr. Nabil Ebraheim
Osteoid Osteoma - Everything You Need To Know - Dr. Nabil Ebraheim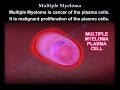 Multiple Myeloma - Everything You Need To Know - Dr. Nabil Ebraheim
Multiple Myeloma - Everything You Need To Know - Dr. Nabil Ebraheim Benign Bone Tumors Made Simple
Benign Bone Tumors Made Simple Anatomy Of The Subscapularis Muscle - Everything You Need To Know - Dr. Nabil Ebraheim
Anatomy Of The Subscapularis Muscle - Everything You Need To Know - Dr. Nabil Ebraheim