Axillary Nerve Injury Shoulder Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describing injury to the axillary nerve associated with shoulder dislocation.
The axillary nerve is the most commonly injured nerve due to shoulder dislocation. It occurs in about 5% of shoulder dislocations. After shoulder dislocation, the patient will be unable to abduct the shoulder, and the deltoid will have no muscle tone.
The supraspinatus muscle will be firing. There will be decreased sensation or absence of sensation on the area of the lateral shoulder. If the patient is older, the inability to abduct the shoulder may be attributed to tear of the rotator cuff, which is common in that age group with shoulder dislocation. This can be a confusing scenario. Rule out a rotator cuff tear. Examine the shoulder sensation.
The intact rotator cuff muscle may abduct the shoulder and confuse the examiner. It is important to check the sensation over the skin of the shoulder. It does not matter if the rotator cuff is intact or torn. The sensation over the skin of the lateral shoulder will tell you if there is axillary nerve palsy or not. Injury of the axillary nerve varies from neuropraxia to complete tear of the nerve.
The axillary nerve passes over the subscapularis and then curves backwards below it and underneath the shoulder joint capsule to enter the quadrangular space.
Within the quadrangular space, the axillary nerve is accompanied by the posterior circumflex humeral artery. This artery is important because it is believed that this artery is the main blood supply to the humeral head. After passing through the quadrangular space, the axillary nerve divides into anterior and posterior divisions. The anterior division curves anterior under the deltoid muscle. The deltoid muscle is innervated by this anterior division of the axillary never. The posterior division supplies the teres minor muscle and the remaining posterior portion of the deltoid muscles as well as the skin over the shoulder. The anterior branch of the axillary nerve is located 5-7 cm distal to the lateral edge of the acromion. Do not exceed deltoid splitting approach more than 5 cm below the acromion or you risk injury to the axillar nerve. During surgery, adduction and external rotation moves the nerve away from the surgical field.
What do you do when the axillary nerve is injured?
• Give the patient a sling for comfort.
• Physical therapy
• Follow the patient’s progress clinically (usually the nerve will recover).
• Get EMG and nerve studies
o Biphasic waveforms will be seen at 3-4 weeks if the nerve recovers.
• If the nerve does not recover:
o You will get fibrillation potentials and P-waves.
• Failure to abduct the shoulder after 4-6 months despite physical therapy means that the condition is permanent and the patient may not achieve abduction of the shoulder without recovery of the deltoid muscle (too late for deltoid to recover).
• Since the intact rotator cuff muscle failed to abduct the shoulder and to take over the job of the deltoid muscle, then this condition is permanent.
When the condition is permanent you have two options:
• Exploration of the nerve for release, repair, or reconstruction of the nerve (reconstructed by a nerve graft).
• Do a tendon transfer.
o Transfer of the trapezius to the proximal humerus.
o The result of this transfer is usually poor.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundation/home/Give_Online.aspx?sig=29
Видео Axillary Nerve Injury Shoulder Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
The axillary nerve is the most commonly injured nerve due to shoulder dislocation. It occurs in about 5% of shoulder dislocations. After shoulder dislocation, the patient will be unable to abduct the shoulder, and the deltoid will have no muscle tone.
The supraspinatus muscle will be firing. There will be decreased sensation or absence of sensation on the area of the lateral shoulder. If the patient is older, the inability to abduct the shoulder may be attributed to tear of the rotator cuff, which is common in that age group with shoulder dislocation. This can be a confusing scenario. Rule out a rotator cuff tear. Examine the shoulder sensation.
The intact rotator cuff muscle may abduct the shoulder and confuse the examiner. It is important to check the sensation over the skin of the shoulder. It does not matter if the rotator cuff is intact or torn. The sensation over the skin of the lateral shoulder will tell you if there is axillary nerve palsy or not. Injury of the axillary nerve varies from neuropraxia to complete tear of the nerve.
The axillary nerve passes over the subscapularis and then curves backwards below it and underneath the shoulder joint capsule to enter the quadrangular space.
Within the quadrangular space, the axillary nerve is accompanied by the posterior circumflex humeral artery. This artery is important because it is believed that this artery is the main blood supply to the humeral head. After passing through the quadrangular space, the axillary nerve divides into anterior and posterior divisions. The anterior division curves anterior under the deltoid muscle. The deltoid muscle is innervated by this anterior division of the axillary never. The posterior division supplies the teres minor muscle and the remaining posterior portion of the deltoid muscles as well as the skin over the shoulder. The anterior branch of the axillary nerve is located 5-7 cm distal to the lateral edge of the acromion. Do not exceed deltoid splitting approach more than 5 cm below the acromion or you risk injury to the axillar nerve. During surgery, adduction and external rotation moves the nerve away from the surgical field.
What do you do when the axillary nerve is injured?
• Give the patient a sling for comfort.
• Physical therapy
• Follow the patient’s progress clinically (usually the nerve will recover).
• Get EMG and nerve studies
o Biphasic waveforms will be seen at 3-4 weeks if the nerve recovers.
• If the nerve does not recover:
o You will get fibrillation potentials and P-waves.
• Failure to abduct the shoulder after 4-6 months despite physical therapy means that the condition is permanent and the patient may not achieve abduction of the shoulder without recovery of the deltoid muscle (too late for deltoid to recover).
• Since the intact rotator cuff muscle failed to abduct the shoulder and to take over the job of the deltoid muscle, then this condition is permanent.
When the condition is permanent you have two options:
• Exploration of the nerve for release, repair, or reconstruction of the nerve (reconstructed by a nerve graft).
• Do a tendon transfer.
o Transfer of the trapezius to the proximal humerus.
o The result of this transfer is usually poor.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundation/home/Give_Online.aspx?sig=29
Видео Axillary Nerve Injury Shoulder Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Nerve injury , Injuries .Complete - Everything You Need To Know - Dr. Nabil Ebraheim
Nerve injury , Injuries .Complete - Everything You Need To Know - Dr. Nabil Ebraheim Axillary Nerve | 3D Anatomy Tutorial
Axillary Nerve | 3D Anatomy Tutorial Axillary Nerve anatomy - Everything You Need To Know - Dr. Nabil Ebraheim
Axillary Nerve anatomy - Everything You Need To Know - Dr. Nabil Ebraheim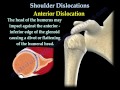 Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim
Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim Shoulder dislocation , Hill Sachs Lesion - Everything You Need To Know - Dr. Nabil Ebraheim
Shoulder dislocation , Hill Sachs Lesion - Everything You Need To Know - Dr. Nabil Ebraheim Lesions Of The Shoulder SLAP Tear - Everything You Need To Know - Dr. Nabil Ebraheim
Lesions Of The Shoulder SLAP Tear - Everything You Need To Know - Dr. Nabil Ebraheim How to test the Axillary Nerve from Brachial Plexus C5 & C6
How to test the Axillary Nerve from Brachial Plexus C5 & C6 Axillary nerve injury evaluation by Paul Marquis PT
Axillary nerve injury evaluation by Paul Marquis PT Axillary nerve Anatomy : Origin, Course, Branches, innervation #Usmle Anatomy
Axillary nerve Anatomy : Origin, Course, Branches, innervation #Usmle Anatomy Radial Nerve Injury,Where Is The Injury - Everything You Need To Know - Dr. Nabil Ebraheim
Radial Nerve Injury,Where Is The Injury - Everything You Need To Know - Dr. Nabil Ebraheim Biceps Tendon Subluxation Or Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim
Biceps Tendon Subluxation Or Dislocation - Everything You Need To Know - Dr. Nabil Ebraheim Flossing the Axillary Nerve - Ask Dr. Abelson
Flossing the Axillary Nerve - Ask Dr. Abelson Shoulder Dislocation: Will It Happen Again? Do You Need Surgery??
Shoulder Dislocation: Will It Happen Again? Do You Need Surgery?? Orthopaedics : Anterior dislocation of shoulder - Marrow Edition 5 (Clinical Core) Sample Video
Orthopaedics : Anterior dislocation of shoulder - Marrow Edition 5 (Clinical Core) Sample Video![The Brachial Plexus II: Animated Review [HD]](https://i.ytimg.com/vi/mKbk_ey_dEs/default.jpg) The Brachial Plexus II: Animated Review [HD]
The Brachial Plexus II: Animated Review [HD] Subscapularis Muscle Tear A Hidden Lesion - Everything You Need To Know - Dr. Nabil Ebraheim
Subscapularis Muscle Tear A Hidden Lesion - Everything You Need To Know - Dr. Nabil Ebraheim Musculocutaneous Nerve - Everything You Need To Know - Dr. Nabil Ebraheim
Musculocutaneous Nerve - Everything You Need To Know - Dr. Nabil Ebraheim Is Your Shoulder Pain From Nerve, Muscle, or Joint? How to Tell (Updated)
Is Your Shoulder Pain From Nerve, Muscle, or Joint? How to Tell (Updated) Diagnosing a shoulder dislocation
Diagnosing a shoulder dislocation Lockdown Anatomy with Prof Alice Roberts #8: Nerves of the Upper Limb
Lockdown Anatomy with Prof Alice Roberts #8: Nerves of the Upper Limb