Hyperkalemia for USMLE Step 1 and USMLE Step 2
PHYSIOLOGY
Normal potassium level is anywhere between 3.5 to 5.0meq per liter. Any amount above this is considered hyperkalemia and any amount below this is considired hypokalemia.
Potassium levels are maintained by the sodium-potassium ATPase pump that maintains more potassium inside the cell rather than outside. The resting membrane potential of excitatory cells is most important such as the muscle and neurons.
When you eat a banana the food goes into the intestine and eventually goes into the blood. Potassium is absorbed with glucose and so insulin helps lower glucose levels, but also maintains low levels of potassium to prevent hyperkalemia.
The muscle has beta 2 receptors and during exercise the muscle release potassium. However, the beta 2 receptors also actiave sodium potassium ATPase channels also helping prevent hyperkalemia during periods of exercise.
The potassium also makes it way to the adrenal gland and causes release of aldosterone which acts on the principal cells in the distal convulated tubules. On these cells more potassium is released into the urine preventing hyperkalemia by increase sodium channels and increase sodium potassium ATPase channels.
ETIOLOGY PF HYPERKALEMIA
INCREASE POTASSIUM RELEASE FROM CELL CAUSES HYPERKALEMIA
Catabolism - burns, trauma, rhabdomyolysis, tumor lysis syndrome
Cellular Shift - Acidosis, Hyperosmolality, Insulin deficiency,
Drugs - Digitalis, Beta-blockers, RBC Transfusion
DECREASE URINARY EXCRETION CAUSING HYPERKALEMIA
Aldosterone - anything that inhibits aldosterone will cause hyperkalemia
Addison's, Spironolactone, eplereonone, triamterene, amiloride, ACE inhibitors, NSAIDs
RTA Type 4 - Decrease Sodium reabsorption in principal cells. Obstructive uropathy, lupus nephritis, sickle cell disease
Acute Kidney injury - Low GFR and oliguria causes decrease potassium filterin causing hyperkalemia
SPURIOUS CAUSES OF HYPERKALEMIA
Hemolysis, thrombocytosis, leukocytosis, tourniquet
CLINICAL ASPECTS OF HYPERKALEMIA
Muscle weakness - ascending legs, trunks arm
ECG Changes - Hyperacute T waves, No P Waves,
Arrythmias - Sinus bradycardia, V. Tachycardia, Ventricular Fibrillation, Systole, LBBB, RBBB, Bifasicular Block, AV Block
Decease Urine Acid Secretion - Potassium is necessary for Ammonia secretion which is necessary for proton secreiton
MANAGEMENT OF HYPERKALEMI
First check for ECG Changes.
If there is ECG Changes, Potassium greater than 7meq or symptomatic then ive Calcium gluconate right away to stabilize the heart.
Then give IV insulin and glucose. Beta 2 agonist, Diuretic, K Binding resins, Hemodialysis, Sodium Bicarbonate if there is acidosis.
If the hyperkalemia is betwen 5 to 6 than change diet or stop drugs that are causing hyperkalemia.
Видео Hyperkalemia for USMLE Step 1 and USMLE Step 2 канала the study spot
Normal potassium level is anywhere between 3.5 to 5.0meq per liter. Any amount above this is considered hyperkalemia and any amount below this is considired hypokalemia.
Potassium levels are maintained by the sodium-potassium ATPase pump that maintains more potassium inside the cell rather than outside. The resting membrane potential of excitatory cells is most important such as the muscle and neurons.
When you eat a banana the food goes into the intestine and eventually goes into the blood. Potassium is absorbed with glucose and so insulin helps lower glucose levels, but also maintains low levels of potassium to prevent hyperkalemia.
The muscle has beta 2 receptors and during exercise the muscle release potassium. However, the beta 2 receptors also actiave sodium potassium ATPase channels also helping prevent hyperkalemia during periods of exercise.
The potassium also makes it way to the adrenal gland and causes release of aldosterone which acts on the principal cells in the distal convulated tubules. On these cells more potassium is released into the urine preventing hyperkalemia by increase sodium channels and increase sodium potassium ATPase channels.
ETIOLOGY PF HYPERKALEMIA
INCREASE POTASSIUM RELEASE FROM CELL CAUSES HYPERKALEMIA
Catabolism - burns, trauma, rhabdomyolysis, tumor lysis syndrome
Cellular Shift - Acidosis, Hyperosmolality, Insulin deficiency,
Drugs - Digitalis, Beta-blockers, RBC Transfusion
DECREASE URINARY EXCRETION CAUSING HYPERKALEMIA
Aldosterone - anything that inhibits aldosterone will cause hyperkalemia
Addison's, Spironolactone, eplereonone, triamterene, amiloride, ACE inhibitors, NSAIDs
RTA Type 4 - Decrease Sodium reabsorption in principal cells. Obstructive uropathy, lupus nephritis, sickle cell disease
Acute Kidney injury - Low GFR and oliguria causes decrease potassium filterin causing hyperkalemia
SPURIOUS CAUSES OF HYPERKALEMIA
Hemolysis, thrombocytosis, leukocytosis, tourniquet
CLINICAL ASPECTS OF HYPERKALEMIA
Muscle weakness - ascending legs, trunks arm
ECG Changes - Hyperacute T waves, No P Waves,
Arrythmias - Sinus bradycardia, V. Tachycardia, Ventricular Fibrillation, Systole, LBBB, RBBB, Bifasicular Block, AV Block
Decease Urine Acid Secretion - Potassium is necessary for Ammonia secretion which is necessary for proton secreiton
MANAGEMENT OF HYPERKALEMI
First check for ECG Changes.
If there is ECG Changes, Potassium greater than 7meq or symptomatic then ive Calcium gluconate right away to stabilize the heart.
Then give IV insulin and glucose. Beta 2 agonist, Diuretic, K Binding resins, Hemodialysis, Sodium Bicarbonate if there is acidosis.
If the hyperkalemia is betwen 5 to 6 than change diet or stop drugs that are causing hyperkalemia.
Видео Hyperkalemia for USMLE Step 1 and USMLE Step 2 канала the study spot
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Residency | Potassium | @OnlineMedEd
Residency | Potassium | @OnlineMedEd Hyperkalemia - causes, symptoms, diagnosis, treatment, pathology
Hyperkalemia - causes, symptoms, diagnosis, treatment, pathology Hypernatremia for USMLE Step 2
Hypernatremia for USMLE Step 2 Diabetic Ketoacidosis (DKA) Explained Clearly Remastered - DKA Pathophysiology
Diabetic Ketoacidosis (DKA) Explained Clearly Remastered - DKA Pathophysiology MRCP | Hyperkalemia | Lectures by Dr Bhatia
MRCP | Hyperkalemia | Lectures by Dr Bhatia Resuscitation V Cast Hyperkalemia
Resuscitation V Cast Hyperkalemia Sodium and Potassium Metabolism (Renin, Angiotensin, Aldosterone, and ADH)
Sodium and Potassium Metabolism (Renin, Angiotensin, Aldosterone, and ADH)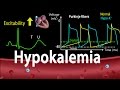 Hypokalemia: Causes, Symptoms, Effects on the Heart, Pathophysiology, Animation.
Hypokalemia: Causes, Symptoms, Effects on the Heart, Pathophysiology, Animation. Hyperkalemia Management & Treatment (Mnemonic) - MEDZCOOL
Hyperkalemia Management & Treatment (Mnemonic) - MEDZCOOL Hyperkalemia Explained Clearly - Fluid and Electrolyte Imbalances
Hyperkalemia Explained Clearly - Fluid and Electrolyte Imbalances Meningitis, Encephalitis, Cerebritis & Cerebral Abscess
Meningitis, Encephalitis, Cerebritis & Cerebral Abscess Hyponatraemia (Hyponatremia) - classification, causes, pathophysiology, treatment
Hyponatraemia (Hyponatremia) - classification, causes, pathophysiology, treatment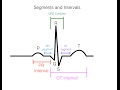 EKG/ECG Interpretation (Basic) : Easy and Simple!
EKG/ECG Interpretation (Basic) : Easy and Simple! Myocardial Infarction and Angina for USMLE Step 1 and USMLE Step 2
Myocardial Infarction and Angina for USMLE Step 1 and USMLE Step 2 Fluid & Electrolytes Nursing Students Hyperkalemia Made Easy NCLEX Review
Fluid & Electrolytes Nursing Students Hyperkalemia Made Easy NCLEX Review Electrolyte Imbalances | Hyperkalemia (High Potassium)
Electrolyte Imbalances | Hyperkalemia (High Potassium) Understanding Hyponatraemia
Understanding Hyponatraemia pH and Acid-Base Balance - Biochemistry
pH and Acid-Base Balance - Biochemistry Hyperkalemia | Etiology, Pathophysiology, Clinical Features, Diagnosis, Treatment
Hyperkalemia | Etiology, Pathophysiology, Clinical Features, Diagnosis, Treatment Hyponatremia Explained Clearly (Remastered) - Electrolyte Imbalances
Hyponatremia Explained Clearly (Remastered) - Electrolyte Imbalances