Glenohumeral Ligaments, ligaments of the shoulder - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim's animated educational video describing the glenohumeral ligaments of the shoulder.
The superior, middle, and inferior glenohumeral ligaments play different roles in the stability of the humeral head, depending on arm position and degree of rotation.
The SGHL runs from the anterosuperior labrum to the humerus.
Function:
Resists anterior translation of adducted arm.
The MGHL runs from the anterosuperior glenoid, arising just inferior o the superior GHL, to the anterior aspect of the anatomic neck of the humerus.
Function: resists anterior and posterior translation in the midrange of arm abduction at 45 degrees and external rotation.
The IGHL (anterior and posterior bands) run from the inferior two-thirds of the glenoid labrum to the lateral humerus.
Function:
Resists anterior-inferior translation of the arm in 90 degrees abduction and external rotation.
The anterior band of the IGHL forms a weak link that predisposes to Bankart lesions. The IGHL (posterior band) resists posterior-inferior translation in adduction and internal rotation. Tightness of the posterior band leads to internal impingement and increased shear forces on the superior labrum.
1.Comma Sign
a.The superolateral margin of the subscapularis is identified by “comma sign” during surgery.
b.The comma sign fibers are oriented perpendicular to the fibers of the subscapularis tendon.
c.The common sign consists of the coracohumeral ligament (CHL), the superior glenohumeral ligament (SGHL), and the medial sling of the biceps.
d.These make one structure that marks the superiorinterval of the lateral subscapularis tendon.
e.These three structures can tear from the humerus, but remain attached to each other.
f.This comma sign helps in identification of the subscapularis tendon during its arthroscopic repair.
2.Buford complex
a.Normal anatomical variant
b.A cord-like middle glenohumeral ligament and absent anterosuperior labrum
c.Looks like a SLAP tear but it is not a SLAP tear.
3.Bankart Lesion
a.Bankart lesion is the most common lesion of anterior shoulder instability following anterior shoulder dislocation
b.It involves avulsion of the anterior inferior labrum.
c.Bankart lesions are typically located in the 3-6 o’clock position because this is where the humeral head dislocates.
d.This is also the area where the anterior band of the inferior glenohumeral ligament inserts.
e.Bankart lesions can be either bony or fibrous.
4.ALPSA Lesions
a.The labral ligament complex is displaced medially and shifted inferiorly.
b.The labrum is displaced by the inferior glenohumeral (IGHL) ligament and the labrum is rolled up like a sleeve with an intact anterior scapular periosteum.
5.GLAD Lesion
a.GLAD lesion is a tear of the anterior inferior labrum (non-displaced) with avulsion of the adjacent glenoid cartilage.
b.This lesion results from impaction of the humeral head against the glenoid. This is caused by abduction and external rotation injury.
c.In the GLAD lesion, the labrum is not detached and there is no capsular stripping.
6.HAGL Lesion
a.The position of the inferior glenohumeral ligament (IGHL), which is the most important and strongest ligament, limits anterior/inferior subluxation of the humeral head.
b.Humeral avulsion of the glenohumeral ligament (HAGL) may occur due to shoulder dislocation.
c.The inferior glenohumeral ligament avulses from the inferior humeral neck (HAGL lesion)
d.HAGL lesions usually occur due to anterior shoulder dislocation caused by combined hyperabduction and external rotation of the arm.
e.It looks like the capsule and the ligament is avulsed from the inferior humeral neck and ripped off.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundation/home/Give_Online.aspx?sig=29
Видео Glenohumeral Ligaments, ligaments of the shoulder - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
The superior, middle, and inferior glenohumeral ligaments play different roles in the stability of the humeral head, depending on arm position and degree of rotation.
The SGHL runs from the anterosuperior labrum to the humerus.
Function:
Resists anterior translation of adducted arm.
The MGHL runs from the anterosuperior glenoid, arising just inferior o the superior GHL, to the anterior aspect of the anatomic neck of the humerus.
Function: resists anterior and posterior translation in the midrange of arm abduction at 45 degrees and external rotation.
The IGHL (anterior and posterior bands) run from the inferior two-thirds of the glenoid labrum to the lateral humerus.
Function:
Resists anterior-inferior translation of the arm in 90 degrees abduction and external rotation.
The anterior band of the IGHL forms a weak link that predisposes to Bankart lesions. The IGHL (posterior band) resists posterior-inferior translation in adduction and internal rotation. Tightness of the posterior band leads to internal impingement and increased shear forces on the superior labrum.
1.Comma Sign
a.The superolateral margin of the subscapularis is identified by “comma sign” during surgery.
b.The comma sign fibers are oriented perpendicular to the fibers of the subscapularis tendon.
c.The common sign consists of the coracohumeral ligament (CHL), the superior glenohumeral ligament (SGHL), and the medial sling of the biceps.
d.These make one structure that marks the superiorinterval of the lateral subscapularis tendon.
e.These three structures can tear from the humerus, but remain attached to each other.
f.This comma sign helps in identification of the subscapularis tendon during its arthroscopic repair.
2.Buford complex
a.Normal anatomical variant
b.A cord-like middle glenohumeral ligament and absent anterosuperior labrum
c.Looks like a SLAP tear but it is not a SLAP tear.
3.Bankart Lesion
a.Bankart lesion is the most common lesion of anterior shoulder instability following anterior shoulder dislocation
b.It involves avulsion of the anterior inferior labrum.
c.Bankart lesions are typically located in the 3-6 o’clock position because this is where the humeral head dislocates.
d.This is also the area where the anterior band of the inferior glenohumeral ligament inserts.
e.Bankart lesions can be either bony or fibrous.
4.ALPSA Lesions
a.The labral ligament complex is displaced medially and shifted inferiorly.
b.The labrum is displaced by the inferior glenohumeral (IGHL) ligament and the labrum is rolled up like a sleeve with an intact anterior scapular periosteum.
5.GLAD Lesion
a.GLAD lesion is a tear of the anterior inferior labrum (non-displaced) with avulsion of the adjacent glenoid cartilage.
b.This lesion results from impaction of the humeral head against the glenoid. This is caused by abduction and external rotation injury.
c.In the GLAD lesion, the labrum is not detached and there is no capsular stripping.
6.HAGL Lesion
a.The position of the inferior glenohumeral ligament (IGHL), which is the most important and strongest ligament, limits anterior/inferior subluxation of the humeral head.
b.Humeral avulsion of the glenohumeral ligament (HAGL) may occur due to shoulder dislocation.
c.The inferior glenohumeral ligament avulses from the inferior humeral neck (HAGL lesion)
d.HAGL lesions usually occur due to anterior shoulder dislocation caused by combined hyperabduction and external rotation of the arm.
e.It looks like the capsule and the ligament is avulsed from the inferior humeral neck and ripped off.
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Donate to the University of Toledo Foundation Department of Orthopaedic Surgery Endowed Chair Fund:
https://www.utfoundation.org/foundation/home/Give_Online.aspx?sig=29
Видео Glenohumeral Ligaments, ligaments of the shoulder - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Lesions Of The Shoulder SLAP Tear - Everything You Need To Know - Dr. Nabil Ebraheim
Lesions Of The Shoulder SLAP Tear - Everything You Need To Know - Dr. Nabil Ebraheim Glenohumeral joint: Structure and actions
Glenohumeral joint: Structure and actions Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim
Rotator Cuff Muscles - Everything You Need To Know - Dr. Nabil Ebraheim Shoulder Joint: Movements, Bones & Muscles - Human Anatomy | Kenhub
Shoulder Joint: Movements, Bones & Muscles - Human Anatomy | Kenhub Systematic Interpretation of Shoulder MRI: How I do it
Systematic Interpretation of Shoulder MRI: How I do it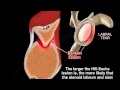 Shoulder dislocation , Hill Sachs Lesion - Everything You Need To Know - Dr. Nabil Ebraheim
Shoulder dislocation , Hill Sachs Lesion - Everything You Need To Know - Dr. Nabil Ebraheim The Rotator Cuff
The Rotator Cuff Internal Impingement of the shoulder- Everything You Need To Know - Dr. Nabil Ebraheim
Internal Impingement of the shoulder- Everything You Need To Know - Dr. Nabil Ebraheim Shoulder Impingement - Dr. Richard Hawkins
Shoulder Impingement - Dr. Richard Hawkins Shoulder Exam (7 of 9): Exam to detect a SLAP tear
Shoulder Exam (7 of 9): Exam to detect a SLAP tear Lesions Of The Shoulder HAGL Lesion - Everything You Need To Know - Dr. Nabil Ebraheim
Lesions Of The Shoulder HAGL Lesion - Everything You Need To Know - Dr. Nabil Ebraheim Rotator Cuff Tears: What Is the Evidence? - Brian Feeley, MD
Rotator Cuff Tears: What Is the Evidence? - Brian Feeley, MD 2 Glenohumeral Joint Capsule & Ligaments
2 Glenohumeral Joint Capsule & Ligaments Ligaments of the Elbow Stability Of The Elbow - Everything You Need To Know - Dr. Nabil Ebraheim
Ligaments of the Elbow Stability Of The Elbow - Everything You Need To Know - Dr. Nabil Ebraheim Biomechanical Summary of Reverse Shoulder Arthroplasty
Biomechanical Summary of Reverse Shoulder Arthroplasty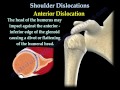 Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim
Shoulder Dislocations ,Everything You Need To Know - Dr. Nabil Ebraheim How to read your shoulder MRI
How to read your shoulder MRI Shoulder Impingement Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim
Shoulder Impingement Syndrome - Everything You Need To Know - Dr. Nabil Ebraheim Arthroscopic Bankart Repair
Arthroscopic Bankart Repair Biceps Tendon Pathology - Everything You Need To Know - Dr. Nabil Ebraheim
Biceps Tendon Pathology - Everything You Need To Know - Dr. Nabil Ebraheim