Pediatric Cervical Spine Injuries - Everything You Need To Know - Dr. Nabil Ebraheim
Dr. Ebraheim’s educational animated video describes the Cervical Spine injuries in Pediatrics.
Spinal Cord Injury Without Radiological Abnormalities (SCIWORA) is due to ligaments elasticity and flexibility of the pediatric vertebral column which can withstand injuries without evidence of deformity, however, the spinal cord will be damaged. SCIWORA should be suspected in a child with neck injury and neurological symptoms with no radiological bony abnormalities.
Common in spinal cord injuries below 8 years of age.
Usually occurs in the cervical or thoracic spine.
Investigation of choice is MRI.
Treatment by cervical immobilization
SCIWORA usually resolves with no neurological deficiencies but there is high incidence of recurrence.
Younger children less than 10 years due to major trauma leads to more severe injury little potential for recovery.
Older children more than 10 years usually due to sports-related trauma or minor falls leads to transient neuropraxia rapid resolution.
Atlantooccipital dislocation: fatal injury due to major trauma. More common in children than adults.
Diagnosis by X-ray and CT scan. MRI will show ligaments injury
Treatment
Post-reduction radiograph should be obtained to ensure adequate reduction
Cervical spine x-ray should be done daily to ensure maintained reduction
Atalatno occipital dislocation is a ligamentous injury that is usually unstable and may need atlanto-occipital fusion.
Os odontoid is due to congenital or unrecognized fracture of the odontoid. Is accidentally discovered on radiological investigation. It should be differentiated from acute odontoid fractures. Round/oval shaped sclerotic edges. Widely spaced from base of odontoid.
Dens fracture: odontoid is persevered, sharp edges and narrow gap to the base of odontoid.
•Conservative treatment: no pain, no neurological deficiency, no cervical instability.
•Surgery is done in patients with progressive symptoms (neck pain, neurological deficiency or cervical spine instability)
Signs of cervical spine instability
In young children without progressive deficits it is better to delay surgical treatment until six to seven years of age. By that time the child will have sufficient bony development of the cervical spine.
Odontoid fractures occur in young children usually around 4 years of age. C2 synchondrosis (similar to Salter Harris type I).
Persistence of the basilar odontoid synchondrosis is normally seen in one half of all children up to age eleven and may mimic an odontoid fracture. This line appears sclerotic unlike acute fractures and is located well below the base of the odontoid where most adult fractures occur.
Atlanto axial rotatory subluxation
Child with rotatory subluxation of C1 on C2 marked by the direction of head tilt and rotation of the neck.
Signs and symptoms
This injury may be missed due to mild signs and symptoms. The child usually presents with neck pain and torticollis (cock-robin sign). Rule out any neurological deficiencies.
Diagnosis: lateral x-ray anterior displacement of C1 over C2 •Open mouth view x-ray shows asymmetrical lateral masses of C1 •Dynamic CT scan is diagnostic
Treatment: Depends on the duration of injury •For injuries of less than 1 week, immobilization by neck collar should be attempted •Halter traction is used in injuries of more than 1-week duration •Surgical reduction in C1-C2 fusion is used to create fixed deformities or use din patients with neurological deficits.
•Posterior ligamentous disruption: due to flexion or distraction injuries. Maybe missed on radiological evaluation due to normal loss of cervical lordosis in children. Widening of the interspinous space shows the injury on x-ray. MRI is diagnostic for the ligamentous injury. Treatment by immobilization In extension or posterior arthrodesis if signs of instability are present.
•Compression fractures: due to flexion and axial loading injuries. Leads to loss of the vertebral body height. Usually diagnosed on lateral view x-ray. In children under 8 years of age, vertebral height will be gained during growth and kyphosis will be corrected. If hypnosis is more than 20 degrees it might not be corrected with growth.
•Burst fractures: due to axial loading injuries. Treated by traction followed by halo immobilization if there is no neurological deficiency. Surgical fusion is done when neurological deficiencies are present. Anterior fusion can lead to kyphotic deformity due to suppression of the anterior growth potential.
Scoliosis is the lateral curving of the spine. Pediatric spinal cord trauma will almost always result in scoliosis.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Pediatric Cervical Spine Injuries - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Spinal Cord Injury Without Radiological Abnormalities (SCIWORA) is due to ligaments elasticity and flexibility of the pediatric vertebral column which can withstand injuries without evidence of deformity, however, the spinal cord will be damaged. SCIWORA should be suspected in a child with neck injury and neurological symptoms with no radiological bony abnormalities.
Common in spinal cord injuries below 8 years of age.
Usually occurs in the cervical or thoracic spine.
Investigation of choice is MRI.
Treatment by cervical immobilization
SCIWORA usually resolves with no neurological deficiencies but there is high incidence of recurrence.
Younger children less than 10 years due to major trauma leads to more severe injury little potential for recovery.
Older children more than 10 years usually due to sports-related trauma or minor falls leads to transient neuropraxia rapid resolution.
Atlantooccipital dislocation: fatal injury due to major trauma. More common in children than adults.
Diagnosis by X-ray and CT scan. MRI will show ligaments injury
Treatment
Post-reduction radiograph should be obtained to ensure adequate reduction
Cervical spine x-ray should be done daily to ensure maintained reduction
Atalatno occipital dislocation is a ligamentous injury that is usually unstable and may need atlanto-occipital fusion.
Os odontoid is due to congenital or unrecognized fracture of the odontoid. Is accidentally discovered on radiological investigation. It should be differentiated from acute odontoid fractures. Round/oval shaped sclerotic edges. Widely spaced from base of odontoid.
Dens fracture: odontoid is persevered, sharp edges and narrow gap to the base of odontoid.
•Conservative treatment: no pain, no neurological deficiency, no cervical instability.
•Surgery is done in patients with progressive symptoms (neck pain, neurological deficiency or cervical spine instability)
Signs of cervical spine instability
In young children without progressive deficits it is better to delay surgical treatment until six to seven years of age. By that time the child will have sufficient bony development of the cervical spine.
Odontoid fractures occur in young children usually around 4 years of age. C2 synchondrosis (similar to Salter Harris type I).
Persistence of the basilar odontoid synchondrosis is normally seen in one half of all children up to age eleven and may mimic an odontoid fracture. This line appears sclerotic unlike acute fractures and is located well below the base of the odontoid where most adult fractures occur.
Atlanto axial rotatory subluxation
Child with rotatory subluxation of C1 on C2 marked by the direction of head tilt and rotation of the neck.
Signs and symptoms
This injury may be missed due to mild signs and symptoms. The child usually presents with neck pain and torticollis (cock-robin sign). Rule out any neurological deficiencies.
Diagnosis: lateral x-ray anterior displacement of C1 over C2 •Open mouth view x-ray shows asymmetrical lateral masses of C1 •Dynamic CT scan is diagnostic
Treatment: Depends on the duration of injury •For injuries of less than 1 week, immobilization by neck collar should be attempted •Halter traction is used in injuries of more than 1-week duration •Surgical reduction in C1-C2 fusion is used to create fixed deformities or use din patients with neurological deficits.
•Posterior ligamentous disruption: due to flexion or distraction injuries. Maybe missed on radiological evaluation due to normal loss of cervical lordosis in children. Widening of the interspinous space shows the injury on x-ray. MRI is diagnostic for the ligamentous injury. Treatment by immobilization In extension or posterior arthrodesis if signs of instability are present.
•Compression fractures: due to flexion and axial loading injuries. Leads to loss of the vertebral body height. Usually diagnosed on lateral view x-ray. In children under 8 years of age, vertebral height will be gained during growth and kyphosis will be corrected. If hypnosis is more than 20 degrees it might not be corrected with growth.
•Burst fractures: due to axial loading injuries. Treated by traction followed by halo immobilization if there is no neurological deficiency. Surgical fusion is done when neurological deficiencies are present. Anterior fusion can lead to kyphotic deformity due to suppression of the anterior growth potential.
Scoliosis is the lateral curving of the spine. Pediatric spinal cord trauma will almost always result in scoliosis.
Become a friend on facebook:
http://www.facebook.com/drebraheim
Follow me on twitter:
https://twitter.com/#!/DrEbraheim_UTMC
Видео Pediatric Cervical Spine Injuries - Everything You Need To Know - Dr. Nabil Ebraheim канала nabil ebraheim
Показать
Комментарии отсутствуют
Информация о видео
Другие видео канала
 Cervical Spine Trauma - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Spine Trauma - Everything You Need To Know - Dr. Nabil Ebraheim Overview Of Fractures In The Pediatric Age Group
Overview Of Fractures In The Pediatric Age Group Cervical Vertebrae Anatomy || 3D #OMT #COMLEX
Cervical Vertebrae Anatomy || 3D #OMT #COMLEX Whiplash Injuries Causes & Symptoms - Everything You Need To Know - Dr. Nabil Ebraheim
Whiplash Injuries Causes & Symptoms - Everything You Need To Know - Dr. Nabil Ebraheim Cervical Spine Trauma- Operative and Non-Operative Management - David O. Okonkwo, MD, PhD
Cervical Spine Trauma- Operative and Non-Operative Management - David O. Okonkwo, MD, PhD Spinal Cord Injury | Levels of injury
Spinal Cord Injury | Levels of injury Monteggia Fractures In Children
Monteggia Fractures In Children Debate (1) Atlantoaxial instability is the cause of Chiari malformation - Atul Goel
Debate (1) Atlantoaxial instability is the cause of Chiari malformation - Atul Goel Tendon Ruptures Around The Shoulder - Everything You Need To Know - Dr. Nabil Ebraheim
Tendon Ruptures Around The Shoulder - Everything You Need To Know - Dr. Nabil Ebraheim Upper Cervical Spine Trauma - Jens R. Chapman, M.D.
Upper Cervical Spine Trauma - Jens R. Chapman, M.D. Self Treatment Hyperextended Atlas in Upper Cervical Spine
Self Treatment Hyperextended Atlas in Upper Cervical Spine Spinal Trauma: Cervical Trauma Protocol, Common Spinal Fractures – Radiology | Lecturio
Spinal Trauma: Cervical Trauma Protocol, Common Spinal Fractures – Radiology | Lecturio Physical Exam of the Cervical Spine - Dr. Timothy McHenry
Physical Exam of the Cervical Spine - Dr. Timothy McHenry General Trauma Management,the injured patient- Everything You Need To Know - Dr. Nabil Ebraheim
General Trauma Management,the injured patient- Everything You Need To Know - Dr. Nabil Ebraheim Cervical Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim
Cervical Radiculopathy - Everything You Need To Know - Dr. Nabil Ebraheim Cauda Equina Syndrome - Everything You Need To Know - Dr. Nabil
Cauda Equina Syndrome - Everything You Need To Know - Dr. Nabil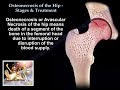 Osteonecrosis Of The Hip Stages & Treatment - Everything You Need To Know - Dr. Nabil
Osteonecrosis Of The Hip Stages & Treatment - Everything You Need To Know - Dr. Nabil Spinal Cord Injury, Detailed - Everything You Need To Know - Dr. Nabil Ebraheim
Spinal Cord Injury, Detailed - Everything You Need To Know - Dr. Nabil Ebraheim Cervical Spine Examination | Practical Clinical Examination Skills
Cervical Spine Examination | Practical Clinical Examination Skills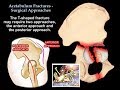 Acetabulum Fractures Surgical Approaches - Everything You Need To Know - Dr. Nabil Ebraheim
Acetabulum Fractures Surgical Approaches - Everything You Need To Know - Dr. Nabil Ebraheim